
FibroScan
My Experience with It
By Angie from @diagnosis_cirrhosis on TikTok
A FibroScan may or may not be part of your story.
That is the first thing to know.
Because with cirrhosis, it is very easy to hear about one test, one number, one scan, one acronym, and suddenly feel like everyone else got handed the secret liver syllabus and you missed class that day.
But FibroScan is not always the main character.
For a lot of people, especially people moving through fatty liver disease, MASLD, NASH, fibrosis tracking, or early cirrhosis staging, FibroScan can be a huge deal. It can be the number. The thing they are watching. The thing that tells them whether their liver is softening, stiffening, improving, protesting, rioting, or generally making a scene.
For me, it was different.
I basically showed up to cirrhosis with the whole punch card already filled out.
Yellow? Check.
Ascites? Check.
Varices? Check.
Portal hypertension acting like it owned the building? Check.
By the time I entered the system, my liver was not whispering, “Maybe we should investigate.” It was standing on a conference table with a megaphone yelling, “We have arrived.”
So when FibroScan came into my life, it was not presented to me as this dramatic diagnostic crossroads. My doctors already knew I had cirrhosis. They already knew it was advanced. They already knew my liver was not exactly giving fresh sponge cake energy.
But I still wanted the information.
I wanted the number.
I wanted the printout.
I wanted one more piece of proof that could help me understand what was happening inside my body without someone cutting into it.
Because that is the thing about cirrhosis: sometimes you are desperate for anything that turns the invisible into something you can point at.
In my state, you can sometimes get FibroScans for free through clinical research organizations like Pinnacle Research Labs. I have gone because, honestly, why not? If someone is offering me a non-invasive look at the little terrorist in my tummy, I am going to take the look.
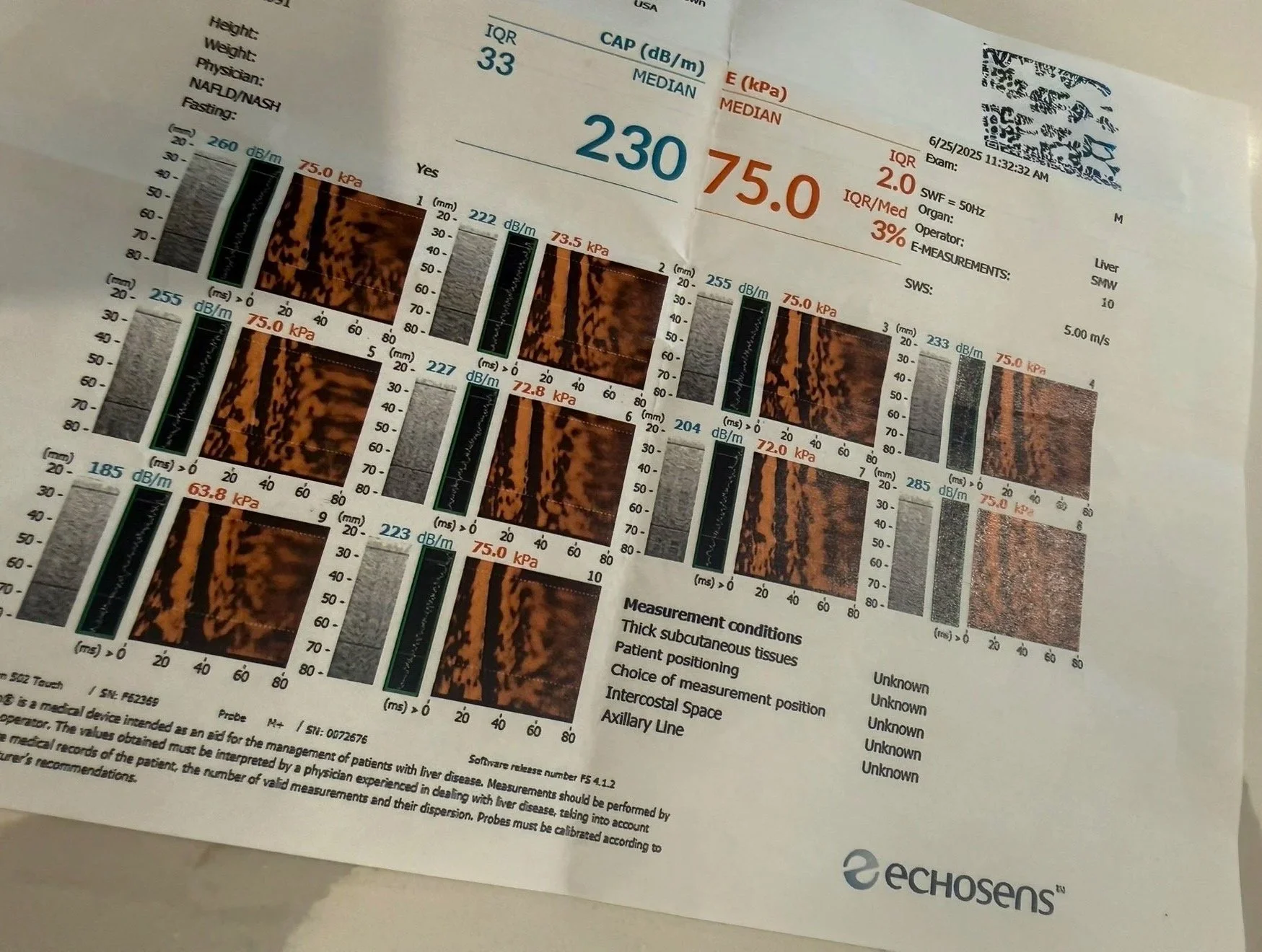
My liver stiffness measurement sits at 75 kPa. And 75 sounds harmless until you understand what it means.
It is not a “high” number.
It is not a “let’s keep an eye on that” number.
It is not a “hmm, interesting” number.
Seventy-five is the ceiling. It is the highest number the machine can physically give you.
So when my result came back as 75, the machine was not saying, “Your liver is stiff.”
It was saying, “I have reached the end of my measuring stick.”

Laughing with the technician before a scan
That is a different kind of information.
That is not a number with room around it.
That is not a number with nuance.
That is a wall.
The first time I ever got a FibroScan, the technician thought the machine was broken. She kept moving the probe around, trying again, shifting angles, pressing in different spots, waiting for the reading to make sense.
Then she said, “Hold on, I have to get my boss.”
And let me tell you: when someone scanning your liver leaves the room to get their boss, your soul does not stay politely in your body.
So now there are two of them huddled around the screen, staring at the machine like it had just said something unforgivable.
And I am lying there thinking:
Great.
Fantastic.
My liver has broken the equipment.
But the machine was not broken.
That was the part that stayed with me.
The machine was fine.
My liver was just that scarred.
That dense.
That remodeled.
That far past squishy.
It had reached the place where the test stopped giving me a gradient and started giving me a ceiling.
That is why a FibroScan can be emotionally strange. It is painless. It is fast. It is not invasive. There are no needles. There is no tube. There is no contrast. There is no giant machine yelling at you to hold your breath.
And yet, it can still hit hard.
Because sometimes the most devastating information comes from the simplest test.
A little probe.
A little thump.
A little screen.
A number that does not blink.
That being said, FibroScans can have false readings. That matters. A high number does not always mean you should immediately spiral into the floorboards. Inflammation can affect the reading. Body size can affect the reading. Rib spacing can affect the reading. Severe ascites can make the test impossible. Some people are not good candidates for the machine at all.
So if your result is weird, alarming, confusing, or higher than expected, do not treat the FibroScan like it is the final prophecy carved into stone.
Treat it like a serious data point.
Bring it to your doctor.
Ask what could be affecting it.
Ask whether it lines up with your labs, imaging, symptoms, and history.
And if your doctor is not ordering FibroScans for you, that does not automatically mean something is being missed. Not everyone has this test as part of their regular monitoring. Some people are followed more closely with ultrasound, CT, MRI, bloodwork, transplant evaluations, physical symptoms, or a combination of all of the above.
What the Procedure Is
A FibroScan, clinically known as transient elastography, is a specialized, non-invasive ultrasound-based test used to measure liver stiffness and fat accumulation [1]. The technology works by sending a low-frequency acoustic wave, or “shear wave,” through the skin into the liver tissue [2].
A sensor tracks how fast that wave travels. Because sound waves travel much faster through rigid, scarred structures than through soft, elastic tissue, the machine can calculate the degree of liver hardness [5].
Why This Procedure May Be Recommended
In modern hepatology, a FibroScan is often used as a painless alternative to an invasive physical needle biopsy. A healthcare provider may recommend this procedure to:
Stage liver fibrosis, tracking how far a patient has progressed from early-stage tissue inflammation to advanced cirrhosis [3].
Quantify liver fat, or steatosis, which is important for diagnosing and monitoring metabolic dysfunction-associated steatotic liver disease, also called MASLD or NASH [4].
Monitor treatment effectiveness, allowing clinicians to see if lifestyle changes, weight loss, antiviral medications, or other interventions are reducing liver stiffness over time [3].
Provide baseline screening in clinical trial environments or research facilities to evaluate eligibility for new liver therapies.
What Doctors Are Trying to Learn
Physicians use a FibroScan to gather numerical data about the physical density and health of your liver tissue [2].
The machine tracks two primary measurements:
Liver Stiffness Measurement, or LSM:
This is measured in kilopascals, or kPa, and estimates how stiff or scarred the liver tissue is [3].
Controlled Attenuation Parameter, or CAP:
This is measured in decibels per meter, or dB/m, and estimates the amount of fat accumulation in the liver [3].
By analyzing the LSM score, your doctor is trying to assess the stage of fibrosis, ranging from F0 for no scarring to F4 for established cirrhosis [4]. By looking at the CAP score, they can estimate how much of the liver may be affected by fatty infiltration [2].
Together, these numbers help doctors evaluate the liver’s structural condition without requiring a surgical biopsy sample [3].
How to Prepare
Preparing for a transient elastography session is usually simple, but there are a few rules that help the machine get a cleaner reading.
Fasting Requirements:
You may be asked to fast, meaning no food, liquids, or gum except small sips of water, for at least 3 hours before the test. This helps stabilize blood flow to the liver and improves measurement accuracy [5].
Clothing Selection:
Wear comfortable, loose-fitting clothing that allows easy access to the right side of your chest and upper abdomen, where the ribs protect the liver [2].
Medical Disclosure:
Tell the technician if you have an active pacemaker, defibrillator, are pregnant, or have other implanted medical devices, because these may affect whether certain elastography equipment is appropriate for you [1].
What Happens During It
The procedure takes place in a standard clinic exam room. It requires no needles and is generally painless [5].
You will lie flat on your back on an examination table with your right arm raised behind your head. This opens the spaces between your right ribs so the technician can access the liver area more easily [5].
The technician will apply a small amount of clear, water-soluble gel to the skin over your liver area [1]. They will then place the FibroScan probe against your side and press a button.
Each time the machine takes a measurement, you may feel a mild, sudden flick or thumping sensation on your skin as the acoustic wave is delivered [2]. The machine usually takes about 10 consecutive readings to create an accurate statistical average.
The entire process is often completed in about 5 to 10 minutes.
What Happens After It
Once the technician wipes the remaining gel off your skin, you can sit up immediately [5].
Because no sedatives, numbing agents, contrast dyes, or incisions are used, there is no recovery period. You can leave the clinic, drive yourself home, eat a regular meal, and resume normal daily activities right away [1].
Risks and What to Watch For
A FibroScan carries an exceptionally safe profile with no meaningful physical recovery risk [1].
Completely Non-Invasive:
Because the test uses acoustic vibrations rather than ionizing radiation or needles, there is no risk of bleeding, tissue damage, or radiation exposure [2].
The Risk of Disqualification or False Readings:
The main limitation of a FibroScan is an inaccurate, unreliable, or impossible reading [5].
The acoustic waves cannot travel properly through fluid, meaning active abdominal ascites may block the machine from working [4]. Severe obesity, narrow rib spaces, acute liver inflammation, recent eating, or technical positioning issues can also cause falsely elevated or unreliable stiffness numbers [3].
That is why doctors do not interpret FibroScan results in isolation. They compare the score with bloodwork, symptoms, physical examination, ultrasound, CT, MRI, and the larger clinical picture [3].
What Results May Mean
The FibroScan computer generates a digital printout displaying your LSM and CAP scores [5].
Normal Stiffness Ranges
A healthy, unscarred liver typically registers a stiffness score between 2.0 and 7.0 kPa [2].
Moderate to Advanced Fibrosis
Scores ranging from 7.5 to 11.5 kPa may suggest moderate to severe scarring, depending on the underlying liver condition and the clinical context [4].
Cirrhosis Thresholds
Scores above roughly 12.5 to 14.0 kPa may represent F4 cirrhosis, though exact cutoffs can vary depending on the liver disease being evaluated and the guideline or equipment used [3].
In advanced, long-term structural disease, the score can climb much higher. Some FibroScan devices max out at 75.0 kPa, which signals severe stiffness and dense scar tissue throughout the liver.
CAP Fatty Ranges
A normal CAP score is often under 238 dB/m, while higher scores, especially above 280 dB/m, may suggest more significant fatty liver infiltration [2].
Questions to Ask Your Doctor
To connect the FibroScan results to your actual liver care plan, consider asking:
What were my exact Liver Stiffness Measurement, or LSM, and CAP scores on today’s FibroScan printout?
Do these numbers suggest my liver scarring is stable, improving, or worsening compared with prior testing?
Could anything temporary, like inflammation, recent food intake, fluid retention, or technical difficulty, have affected today’s reading?
Given my ascites history, BMI, rib spacing, or other factors, do you consider FibroScan an accurate tracking tool for me?
Should we rely more heavily on MRI, CT, ultrasound, labs, or transplant-center evaluation to monitor my cirrhosis?
How often should we repeat FibroScan, if at all, based on my current stage of liver disease?
Sources
[1] Mayo Clinic: Transient Elastography, FibroScan, Overview, Sound Wave Mechanics, and Patient Safety
[2] Cleveland Clinic: Understanding FibroScan Scores, Liver Stiffness Measurements, and Fatty Attenuation
[3] Journal of Hepatology: EASL Clinical Practice Guidelines — Non-Invasive Staging, Transient Elastography Thresholds, and Fibrosis Monitoring in Chronic Liver Disease
[4] The American Journal of Gastroenterology: ACG Clinical Practice Guidance — Role of Elastography in Staging MASLD/NASH and Assessing Advanced Hepatic Cirrhosis
[5] National Institutes of Health / MedlinePlus: FibroScan Protocols, Fasting Preparations, False Reading Variables, and Clinical Interpretations