
AST

@diagnosis_cirrhosis 🧪⚡ AST explained: the lab that says “something’s getting hurt” 👀💥 why is my doctor checking AST? 🤔 what does a high AST mean? 📈 is AST liver damage? 🫀 why is AST high but ALT isn’t? ❓ can exercise raise AST? 💪 why do doctors compare AST vs ALT? ⚖️ AST lives in more than one place 🧬 🫀 liver 💪 muscle ❤️ heart so when AST goes up ⬆️ 👉 it means cells are being injured and leaking it out 🩸🧪 that’s why AST can point to the liver… but it does not always mean the liver is the only source ⚠️ — 💥 what it can mean AST can rise with: 🫀 liver injury 💪 muscle breakdown, hard exercise, or muscle injury ❤️ cardiac stress 🔥 inflammation 👉 same lab… different possible sources — ⚖️ why doctors compare AST vs ALT ALT = more liver-specific 🫀 AST = more general ⚡ so when both are up ⬆️ 👉 doctors think more about the liver when AST is higher than ALT 👀 👉 they may think about: 🍷 alcohol-related liver disease 💪 muscle involvement 🧬 other causes outside the liver — 📈 how much does it move AST can: ⬆️ spike when injury is active ⬇️ come down when that injury improves 👉 it reflects active damage, not the full long-term picture by itself — 🧮 why it’s not in MELD MELD measures: 👉 liver function + survival risk AST measures: 👉 cell injury so even if AST is high 📈 it does not always mean advanced liver failure — 💚 why this matters AST tells you: 👉 something in the body is taking a hit but the big question is always: 👉 where is it coming from? — 🧬 causes of liver-related AST elevation fatty liver disease (MASLD / NAFLD / MASH / NASH) 🍩 alcohol-related liver disease 🚫🍷 hepatitis B 🦠 hepatitis C 🦠 autoimmune hepatitis 🔥 primary biliary cholangitis (PBC) 🧬 primary sclerosing cholangitis (PSC) 🧬 hemochromatosis ⚙️ Wilson’s disease 🪙 alpha-1 antitrypsin deficiency 🧩 drug-induced liver injury 💊 👉 but remember… AST is not just a liver lab ⚠️ — 👩⚕️🩺 talk to your doctor if AST is elevated or changing 📈📉 👉 don’t guess the cause 👉 don’t assume it’s only the liver your doctor will look at: 🧪 ALT, bilirubin, ALP, GGT 📊 trends over time 💪 muscle injury / exercise 💊 meds and supplements 🧬 your full history because AST is a clue… not the whole answer 🧩👀 — ✨ real talk AST can look scary because it goes up with damage 📈💥 but on its own it really means: 👉 something is getting hurt and the next step is figuring out what 👀 💚 #bloodwork #phlebotomist #liverhealth #medicaltiktok #fattyliver ♬ original sound - diagnosis cirrhosis
Top 4 AST Need to Knows
Important Medical Disclaimer: I am Angie, a cirrhosis patient sharing my personal lifestyle, nutrition, and mindset journey. I am a data aggregator and community builder, not a licensed medical professional, doctor, or dietitian. Content on diagnosiscirrhosis.com is based solely on my personal experience living with advanced liver disease and is intended for informational and educational purposes only. It does not constitute medical advice or a substitute for professional medical care. Always follow the recommendations of your own healthcare team and consult your hepatologist or physician before changing your diet, medication, or lifestyle routine.
My Experience with It
By Angie from@Diagnosis_Cirrhosis on TikTok
AST is one of those numbers that lives in the medical periphery until it suddenly does not.
You hear it floating around in annual physicals, routine bloodwork, wellness portals, and those lab result pages where half the numbers look like they were named by someone losing a bet. It feels like something you are probably supposed to understand by adulthood, but unless something is actually wrong, you do not really have to.
You see it once a year. Maybe.
The doctor says your labs look fine. You nod like you know what was being measured. You get your flu shot, your little Band-Aid, your vague sense of moral superiority for completing preventive care, and you leave.
AST stays forgettable. Until you get sick.

And when you get sick with cirrhosis, AST stops being background noise and becomes one of the sets of letters you suddenly know by heart.
Then comes the next problem: AST and ALT.
The Tweedledee and Tweedledum of the liver enzyme world.
Everyone mixes them up. Everyone treats them like interchangeable little liver twins, when they actually behave differently and tell doctors slightly different parts of the story.
The way I keep them straight is not medically perfect, but it works for my brain:
ALT = Always Liver.
AST = And Sometimes Liver.
Meaning ALT is more liver-specific, while AST can come from the liver but can also come from other places, especially muscle. So yes, AST can rise after intense exercise. That is technically true.
But here is where I get a little twitchy. Because once you have advanced liver disease, “maybe it was leg day” is not exactly the level of clinical analysis I am looking for.
Could a workout affect AST? Sure.
But when you are living in cirrhosis world, you need more acuity than internet trivia. You need to understand patterns, trends, context, symptoms, timing, and whether a number is making a meaningful move or simply doing the weird little lab-value cirrhosis cha-cha that bodies love to do.
That is a conversation I have with my doctor often: Is this a meaningful change, or is this just noise?
Because AST and ALT are transient. They move. They fluctuate. They can rise and fall for different reasons. A single out-of-range value may matter, or it may need to be interpreted alongside the rest of the picture.
Why Isn't in the MELD ?
@diagnosis_cirrhosis 🧪📊 Why aren’t AST and ALT part of the MELD score? One of the most frustrating things about liver disease is looking at your labs and feeling like the numbers are arguing with each other. Maybe your AST and ALT are sky-high, but your MELD barely moves. Maybe your enzymes improved, but you still feel awful. Maybe you’re wondering why your doctor doesn’t care about ALT and AST for transplant the way you do, or why a MELD score can affect transplant priority while liver enzymes are not even in the calculation. If you’ve ever felt like the numbers are speaking two different languages, you’re not alone. Because they are. — 🚗 Think of AST and ALT as a hail storm. Think of MELD as whether the car still runs. AST and ALT tell you: 🌩️ How hard is the car getting hit right now? MELD tells you: 🚗 Does the engine still work? Those are different questions. — When liver cells are injured, they leak AST and ALT into the bloodstream. That can happen with viral hepatitis, autoimmune hepatitis, medication injury, alcohol-related hepatitis, or fatty liver inflammation. The hail storm can be enormous. A massive hail storm can crack the windshield, dent every panel, destroy the paint, and make the car look terrible… while the engine still starts perfectly. That’s why people ask: 👉 Why are my ALT and AST high but my MELD score is low? 👉 Why doesn’t a high ALT and AST make my MELD score high? Because injury and function are not the same thing. The liver may be taking a beating, but it may still be functioning. — This is also why transplant teams don’t prioritize based on AST and ALT. It feels strange because higher enzymes seem like they should mean a sicker liver. But transplant is not asking: ❌ How much damage is happening today? It is asking: ⚠️ How likely is this person to die if nothing changes? That is the purpose of MELD. So when people ask: 👉 Why doesn’t my doctor care about ALT and AST for transplant? 👉 Why aren’t enzymes important for mortality risk? The answer is that AST and ALT are good at detecting injury, but much weaker at predicting survival. Someone can have AST and ALT in the thousands from acetaminophen overdose, hepatitis A, acute viral hepatitis, or drug-induced liver injury and still recover completely if the liver keeps functioning. — So why aren’t AST and ALT included in the MELD score? Because MELD was built around mortality risk. It uses: 🟡 bilirubin — can the liver clear waste? 🩸 INR — can the liver make clotting proteins? 🫘 creatinine — are the kidneys still working? 🧂 sodium — how disrupted has circulation become? Those predict survival better than enzymes. — Now flip it around. If my liver is failing, why are my enzymes normal? Because AST and ALT measure active destruction, not remaining capacity. In advanced cirrhosis, there may not be many healthy liver cells left to leak enzymes. So AST and ALT can look normal while bilirubin rises, INR rises, kidney function worsens, sodium falls, and the “engine” is failing. That is what MELD is watching. — And this is why MELD can feel disconnected from real life. If you have a MELD of 9 or 10 and still feel terrible, you are not crazy. MELD does not directly measure ascites, edema, fatigue, weakness, hepatic encephalopathy, or how much cirrhosis has taken over your daily life. So when people ask: 👉 Why doesn’t MELD capture how I actually feel? 👉 Why do I feel terrible if my MELD is low? The answer is that MELD measures mortality risk. Not quality of life. — AST & ALT: 🌩️ How bad is the hail storm? MELD: 🚗 Does the car still run? One measures active injury. One measures remaining function. One measures damage. The other mortality risk. And that’s why they don’t always agree. 👩⚕️👨⚕️🩺 Always talk to your doctor or hepatologist about AST, ALT, bilirubin, INR, creatinine, sodium, MELD score, Child-Pugh score, transplant eligibility, and what those numbers mean in your specific situation. #liverhealth #livertransplant #hepatitis #fattyliver #bloodwork ♬ The Mountain - FASSounds
For many of us, we zero in on our liver enzymes and watch our AST numbers like a hawk, thinking a high number means our disease is progressing and a low number means we are winning.It is completely jarring when you find out that the MELD score—the absolute formula dictating your liver transplant priority list—completely leaves AST out of the math [1].
The clinical reason for this omission comes down to a fundamental concept: AST is a marker of acute cellular injury, not a measure of overall organ failure[2]. An AST spike means cells are actively under stress or bursting open, but it does not tell the transplant calculator how much operational liver factory space you have left to keep you alive over the next three months[3]. The MELD formula is rigidly designed to predict absolute, short-term survival probability.
Because AST levels can fluctuate wildly based on temporary variables—like a strenuous muscle workout or a mild reaction to a new medication—putting it in the equation would introduce too much unpredictable noise and make the ranking system dangerously unfair [4].
Using AST would also trigger massive mathematical errors because of what clinicians call "the cirrhosis paradox" [3]. In advanced, long-term cirrhosis, your liver can become so heavily scarred that it physically lacks functional parenchymal tissue. Because there are simply fewer healthy cells left to open up and leak enzymes, an advanced patient can have an AST number that looks completely normal on paper, despite being in urgent need of a transplant [4].
If the transplant networks relied on AST, stable patients with temporary inflammation would be pushed to the top of the list, while critically ill patients with highly scarred livers would be pushed to the bottom. To prevent this, the algorithm ignores transient cell-death flares entirely and sticks strictly to steady operational metrics that track life-sustaining functions, like your bilirubin and your INR [5].
Key Takeaways:
What the Procedure Is
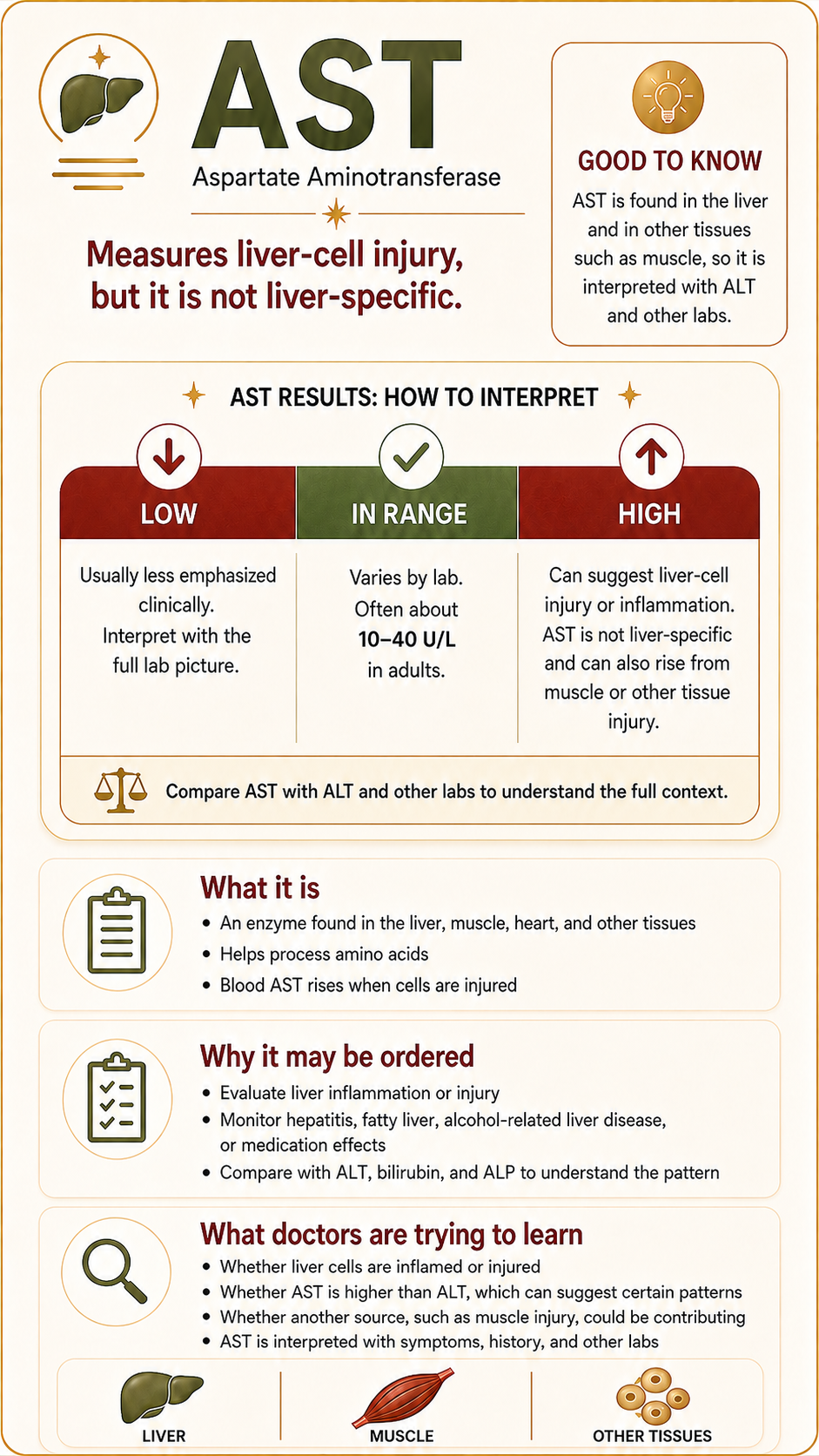
The Aspartate Aminotransferase (AST) test is a routine laboratory procedure that measures the concentration of the AST enzyme circulating in your bloodstream [1]. While AST is found in high amounts within liver cells, it is an enzyme that also lives inside cardiac muscle, skeletal muscle, kidneys, and the brain [2]. When these specific cells experience stress, injury, or active degradation, their cellular membranes become permeable, leaking AST directly into your blood components [2, 5].
Why This Procedure May Be Recommended
A healthcare provider will typically order an AST test as a component of a comprehensive metabolic panel (CMP) or a targeted liver panel [1, 4]. Clinical guidelines from organizations like the American College of Gastroenterology recommend this procedure to [4]:
Evaluate diagnostic symptoms pointing toward hepatic distress, such as jaundice, abdominal distension, dark urine, or uncharacteristic pruritus (itching) [1].
Monitor the progression of chronic hepatic diseases, including viral hepatitis, metabolic dysfunction-associated steatotic liver disease (MASLD), and cirrhosis [2].
Screen for drug-induced liver injury (DILI) if a patient is actively taking medications known to cause liver toxicity, such as high-dose acetaminophen or statins [4].
Assess individuals with elevated risk profiles, including a history of heavy alcohol consumption or potential exposure to bloodborne pathogens [1, 4].
What Doctors Are Trying to Learn
Physicians use the AST test to quantify the current scale of active cellular damage occurring in the body [2]. However, because AST is found in multiple organ systems, hepatologists rarely look at this value in a vacuum; they evaluate it alongside ALT (Alanine Aminotransferase), which is concentrated almost exclusively in the liver [1, 4].
By calculating the AST/ALT ratio, clinicians can better determine the specific root cause of the cellular stress [3]. According to clinical guidelines in the American Journal of Gastroenterology, a ratio where AST is significantly higher than ALT is a classic signature that points toward alcoholic liver disease or advancing fibrosis/cirrhosis, whereas a lower ratio where ALT dominates more frequently points to early-stage viral hepatitis or fatty liver disease [4].
How to Prepare
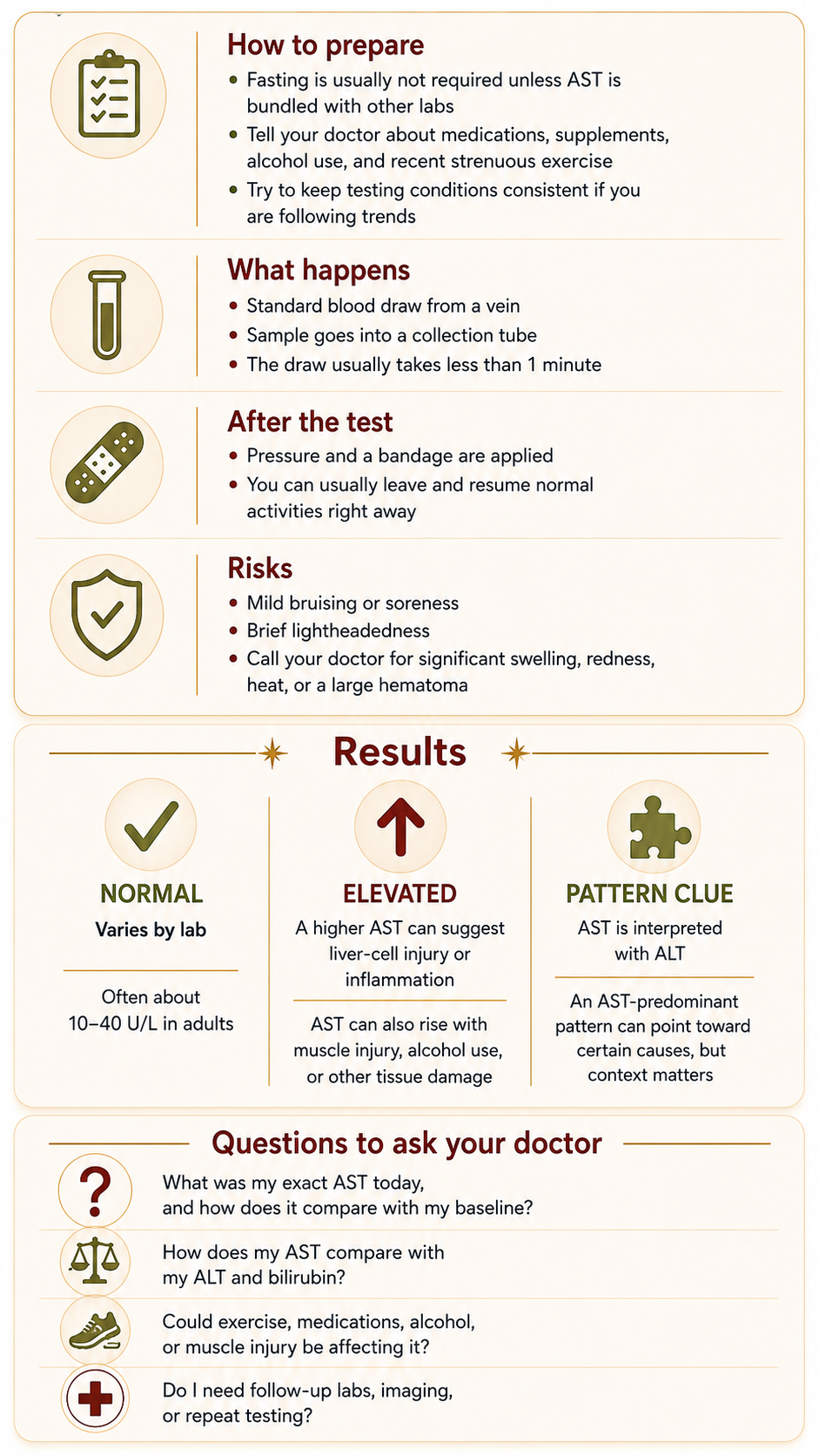
Preparing for an AST blood draw is straightforward, but keeping variables controlled ensures your data isn't skewed:
Fasting Requirements: If the AST test is isolated, fasting is generally unneeded [1]. However, if it is bundled into a broader metabolic panel, your provider will likely mandate an 8-to-12-hour fast.
Medication Disclosures: It is vital to disclose all prescriptions, over-the-counter medications, and herbal supplements, as many common compounds can transiently elevate liver enzymes [4].
Exercise Limitations: Patients are advised to avoid strenuous physical exertion or intense weightlifting directly prior to the draw, as acute skeletal muscle tearing artificially inflates blood AST levels [2, 5].
What Happens During It
The test itself is a standard venipuncture performed by a medical professional [5]. A tourniquet is wrapped around the upper arm to locate the target vein, the skin is sterilized with an antiseptic wipe, and a small needle is inserted to draw blood into a collection tube [5]. The active draw usually concludes in less than 60 seconds [5].
What Happens After It
Following the draw, pressure is applied to the puncture site with a sterile gauze pad, and an adhesive bandage is applied [5]. You can immediately leave the clinical facility, drive yourself home, eat, and resume your typical daily routine [1, 5].
Risks and What to Watch For
An AST blood test carries exceptionally low clinical risk [5]. Minor localized side effects may include [5]:
Mild bruising (ecchymosis) or transient soreness at the venipuncture site.
Brief lightheadedness or vasovagal syncope during or immediately following the needle stick.
Complications to monitor: In incredibly rare instances, localized infection or prolonged bleeding can occur. Patients should contact their provider if they experience worsening localized pain, heat, redness, or swelling [5].
What Results May Mean
While exact reference intervals vary slightly depending on the specific equipment used by an individual laboratory, standard normal ranges typically span 8 to 48 units per liter (U/L) [2].
Normal Range: Suggests a baseline level of cellular turnover without active, widespread tissue damage or severe acute organ inflammation [2].
Mild to Moderate Elevations: Frequently stem from chronic, manageable conditions like fatty liver disease, mild medication-induced stress, or localized muscle trauma [2, 4].
Severe Elevations (10x or greater above normal): Typically indicate acute, sudden hepatic injury, such as acute viral hepatitis or severe toxin exposure like an acetaminophen overdose [1, 2].
The Cirrhosis Paradox: In consensus guidelines published in the Journal of Hepatology, experts emphasize that in cases of long-term, advanced liver disease like cirrhosis, AST and ALT levels can actually fall into near-normal or only mildly elevated ranges [3]. This occurs because extensive parenchymal scarring has replaced healthy tissue, meaning there are simply fewer functional liver cells left to leak enzymes into the blood [3].
Questions to Ask Your Doctor
To help cross-reference your results and guide your next clinical conversation, consider bringing these specific questions to your provider:
What were my precise AST and ALT numbers, and what does the specific ratio between them suggest about my liver health?
Could any of my current daily medications, supplements, or recent physical activities be contributing to these specific numbers?
Given my personal history with cirrhosis, do these numbers represent expected day-to-day fluctuations (noise) or a meaningful trend (signal)?
Do we need to order follow-up diagnostics, such as a hepatic ultrasound, FibroScan, or a comprehensive coagulation panel (PT/INR)?
Are there direct adjustments I should make to my current treatment plan or lifestyle to better support my remaining functional liver tissue?
Sources
[1] Mayo Clinic:Aspartate Aminotransferase (AST) Test Overview & Clinical Purpose
[2] Cleveland Clinic:Understanding AST Levels, Reference Ranges, and Liver Function
[3] Journal of Hepatology: Official Journal of the European Association for the Study of the Liver - Clinical Guidance on Liver Function Test Interpretation
[4] The American Journal of Gastroenterology:ACG Clinical Guideline: Comprehensive Evaluation of Abnormal Liver Chemistries
[5] National Institutes of Health (NIH) / MedlinePlus: AST Blood Test Diagnostics, Procedure Steps, and Risk Factors