
Jaundice
Important Medical Disclaimer: I am Angie, from @diagnosis_cirrhosis on TikTok. I am a cirrhosis patient sharing my personal lifestyle, nutrition, and mindset journey. I am a data aggregator and community builder, not a licensed medical professional, doctor, or dietitian. Content on diagnosiscirrhosis.com is based solely on my personal experience living with advanced liver disease and is intended for informational and educational purposes only. It does not constitute medical advice or a substitute for professional medical care. Always follow the recommendations of your own healthcare team and consult your hepatologist or physician before changing your diet, medication, or lifestyle routine.
Does Jaundice Go Away? Understanding the Yellowing Spectrum in Advanced Liver Disease
By: Angie from @Diagnosis_Cirrhosis on TikTok

Five days after the yellow eyes began
One day you're not yellow. The next day you're standing in front of the bathroom mirror wondering if the lighting has changed (true story: a friend and I once discussed just how amber the lumins of our respective households were).
Maybe it's a faint tint under your tongue. Maybe the whites of your eyes look a little off.
Maybe your urine suddenly resembles something like Dr. Pepper, very medical.
Then, before you know it, the question isn't whether you're jaundiced. It's how yellow you've become. And there’s nothing bellow about it.
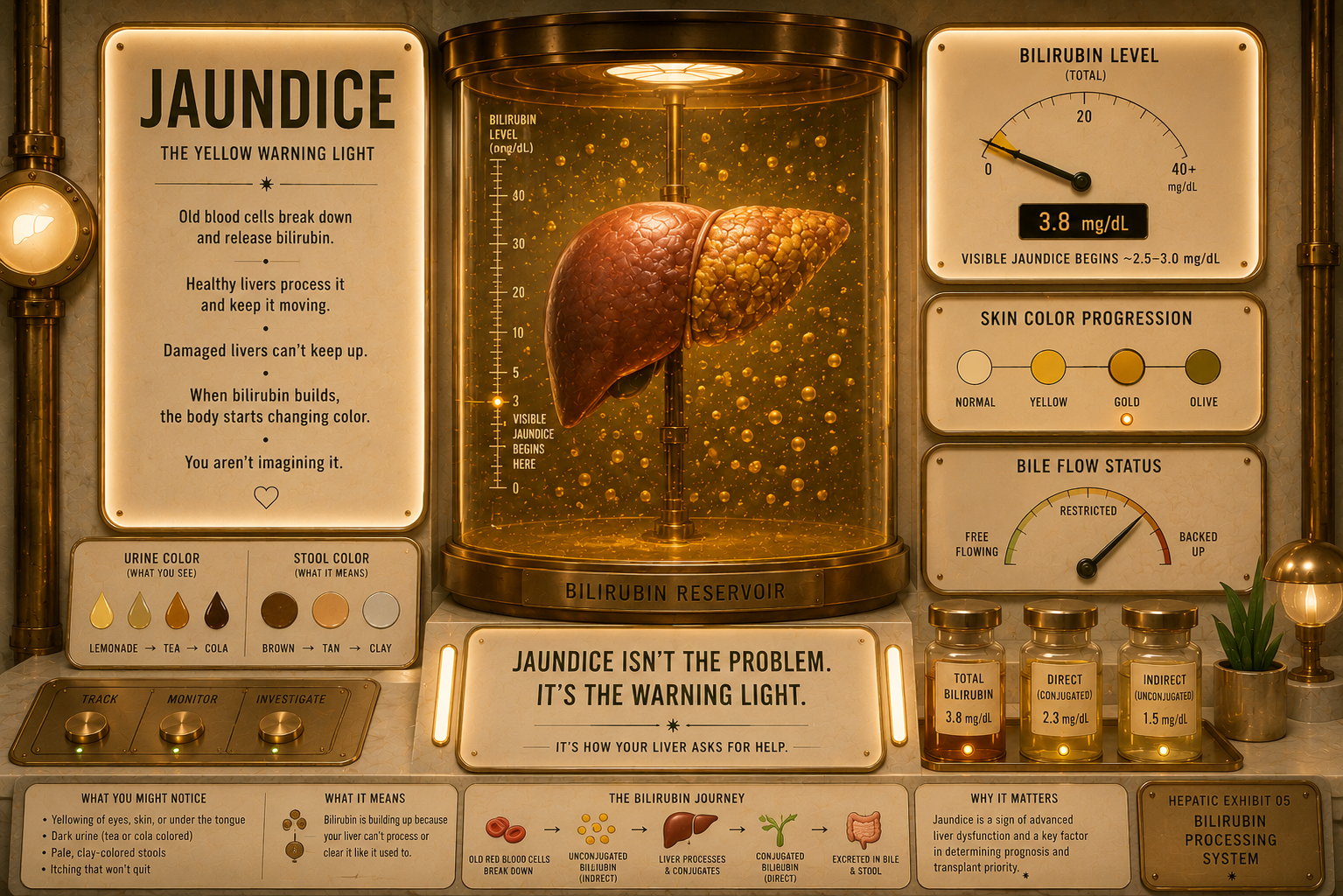
Jaundice is one of the most recognizable signs of advanced liver disease, but what most people don't realize is that it isn't really about the color. The color is just the warning. The real story is what that yellow pigment says about what's happening inside the liver.
Abnormal yellowing in chronic liver failure exists on a highly specific developmental spectrum. Transient (or situational) jaundice is a brief, temporary spike in pigment levels—such as a mild flare after a temporary drug reaction or a passing bout of dehydration—that resolves quickly once the trigger is removed. Hepatic jaundice is an ingrained, systemic failure where a cirrhotic liver’s structural collapse simultaneously destroys its ability to process cellular waste and mechanically blocks the internal plumbing of the bile ducts. [1]
People frequently treat yellowing eyes as a scary but superficial cosmetic pigment issue. In reality, transitioning from a brief, mild tint to true hepatic jaundice marks a critical biological shift, one where your liver tissue has lost its fundamental power to clear old blood cells, pushing your body into a state of active metabolic decompensation. [1]
What It Is
The body's ongoing renewal process requires the spleen to constantly break down old or defective red blood cells, releasing a yellow chemical compound called hemoglobin. The raw byproduct of this process is unconjugated (indirect) bilirubin, which is entirely insoluble in water and must travel to the liver bound tightly to blood proteins [2].
When a patient experiences a brief toxic insult from an over-the-counter drug or a mild infectious flare, it triggers a brief period of transient jaundice. However, as chronic liver disease advances into stage F4 cirrhosis, the internal physics and cellular machinery of the organ collapse. Comprehensive clinical data demonstrates how a scarred liver drives a dual-layer failure of bilirubin processing:
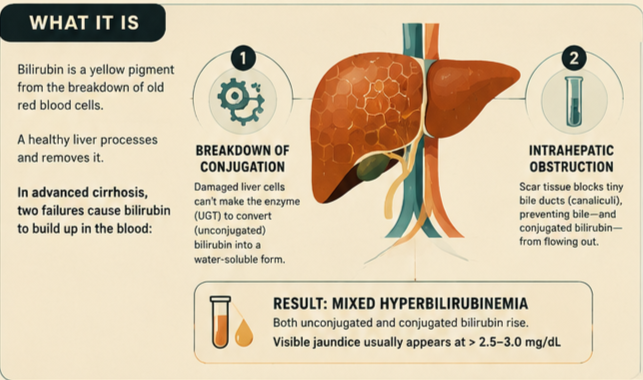
The Breakdown of Conjugation: Damaged liver cells (hepatocytes) lose their ability to manufacture the vital enzyme glucuronyl transferase. Without this enzyme, the liver cannot attach glucuronic acid to the raw pigment, leaving massive amounts of toxic unconjugated bilirubin floating freely in your bloodstream [2].
Intrahepatic Microscopic Obstruction: Simultaneously, the thick bands of rigid collagen scar tissue physically compress and strangle the tiny intrahepatic bile canaliculi. This mechanical bottleneck prevents the liver from exporting the pigment it does manage to process, causing a backup of water-soluble conjugated (direct) bilirubin [3].
The "Mixed Picture" Surge: Because both the chemical factory and the microscopic plumbing collapse at the exact same time, a cirrhotic patient develops a severe, mixed hyperbilirubinemia. Clinical signs of visible jaundice trigger the moment total serum bilirubin levels exceed a threshold of 2.5 to 3.0 mg/dL [4].
The diagnostic line between normal variations and a true hepatic pigment failure is heavily tracked by clinical teams using the classic three-part framework:
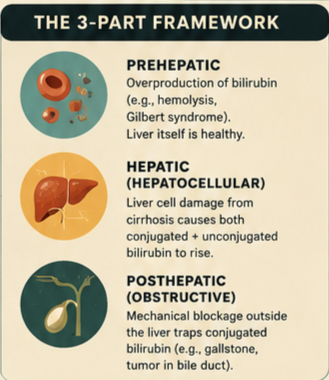
Prehepatic Jaundice: Massive red blood cell destruction (hemolysis) or genetic conditions like Gilbert's syndrome that overwhelm a perfectly healthy liver with unconjugated pigment [5].
Hepatic Jaundice (Hepatocellular): Severe, simultaneous elevation of both conjugated and unconjugated bilirubin caused by structural tissue damage from advanced cirrhosis [5].
Posthepatic Jaundice (Obstructive): A pure mechanical blockage outside the liver, such as a large gallstone or a pancreatic tumor wedged tightly in the common bile duct, trapping pure conjugated bile [5].
What It Feels Like
The physical change and sensory burden of yellowing changes completely as the disease transitions from a passing metabolic lag to advanced structural organ failure.
During Transient Jaundice, you might feel:
A subtle, barely noticeable yellowing underneath your tongue or a slight tint in the corners of your eyes that is only visible under bright, natural daylight.
A fleeting shift that completely fades back to your normal baseline skin tone within a week once you stop a problematic medication or rehydrate your body.
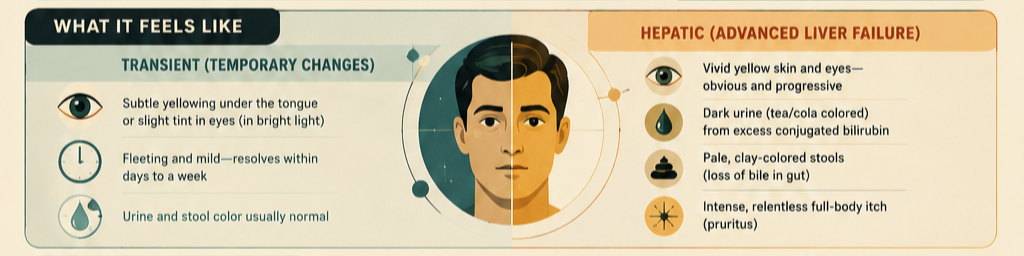
When the condition crosses into Hepatic Jaundice, it looks much different:
A vivid, unmistakable yellowing where your eyes and skin take on a striking golden hue, making you look intensely ill even from across a room [6].
A dramatic change in your restroom routines, where your urine turns a deep, dark brown—almost like black tea or cola—because your kidneys are desperately trying to filter the excess water-soluble pigment out of your blood [6].
The presentation of pale, clay-colored, or "putty-like" stools because the mechanical block inside your scarred liver is entirely stopping bile from entering your digestive tract, stripping your bowel movements of their natural brown color [6].
A relentless, maddening, and deep-seated full-body itch (pruritus) that feels like it is burning from inside your bones, driven by toxic bile salts backing up into your skin tissue alongside the yellow pigment [1].
The Crossover Point: Activating the Decompensation
The transition from a stable, normal bilirubin count to true hepatic jaundice represents an absolute clinical "crossover point." In the timeline of advanced liver disease, crossing this pigment boundary means the patient has officially transitioned from compensated cirrhosis to decompensated cirrhosis [1].
To visualize this crossover point, think of three concrete examples:
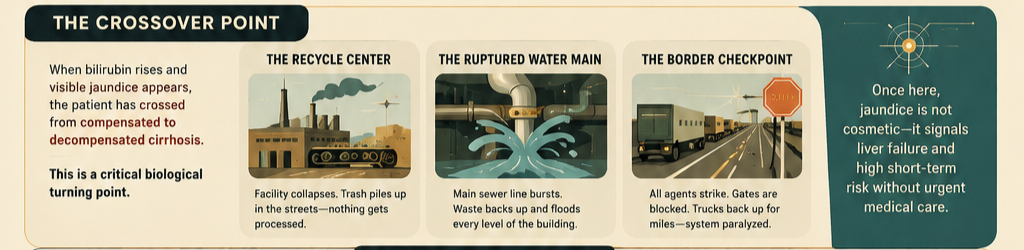
The Backed-Up City Recycling Center: In transient jaundice, the city’s recycling center is simply dealing with an unexpected holiday rush of cardboard boxes (a minor infection or extra medication). The yard gets messy for a weekend, but the workers eventually catch up. The hepatic jaundice crossover point occurs when the main processing building completely collapses. The conveyor belts tear apart, and the sorting machines catch fire; thousands of tons of raw trash pile up in the surrounding streets, entirely blocking traffic because the center can no longer process a single item.
The Ruptured Water Main: Imagine a massive skyscraper with an intricate network of plumbing pipes. In early liver stages, a minor leak causes a small puddle in a maintenance closet. The hepatic crossover point is equivalent to the main sewer line passing through the center of the building completely bursting open. The waste fluid can no longer drop down the drain; it reverses direction, erupting out of the sinks, drinking fountains, and floor boards on every single level, destroying the building’s foundation.
The Overloaded Border Checkpoint: Think of a strict border crossing where trucks must wait to have their cargo manifests certified before entering a new country—this is your liver cells conjugating bilirubin. A transient jam is a passing line on a busy Friday afternoon. The hepatic crossover point is equivalent to a sudden strike where all border agents walk off the job indefinitely and block the gates with concrete barriers. The trucks stack up bumper-to-bumper for hundreds of miles backward into the highways, paralyzing the entire transportation network of the country.
Clinical indicators universally establish that once a patient passes this structural crossover point, the jaundice cannot be dismissed as a minor cosmetic issue. It is a sensory warning sign that the liver's remaining functional tissue can no longer maintain basic survival chemistry, drastically reducing short-term survival probability without aggressive, specialized medical stabilization [1].
Things Nobody Explains

1. Jaundice Frequently Starts in the Mouth Long Before the Eyes Turn Yellow Many patients constantly stare into the bathroom mirror checking the white parts of their eyes (sclera) to see if their liver is failing. Nobody explains that the early stages of jaundice are incredibly subtle and usually start under the tongue or on the soft palate of the mouth [6]. By the time the yellow tint becomes obvious across your facial skin, your blood bilirubin levels have already been elevated for quite some time. [1]
2. The Color Can Change Based on Your Underlying Liver Disease While most people think of jaundice as a standard bright yellow color, the exact shade can vary depending on your specific liver pathology. Patients with a severe biliary obstruction or autoimmune liver disease often develop a dark, greenish-bronze tint. This occurs because the trapped bilirubin sits in the tissue so long that it oxidizes into biliverdin—a deep green pigment that gives the skin a muddy, olive-like appearance [4].
3. Jaundice is a Major Clinical Reason You Are Banned From General Surgery Many patients assume that if they need an unrelated abdominal operation, their doctor can just proceed normally despite their yellow eyes. Nobody explains that active hepatic jaundice is a massive red flag that often completely contraindicates elective surgery [1]. Because a yellow liver cannot synthesize blood-clotting proteins or process anesthesia safely, undergoing general surgery with active jaundice carries an unacceptably high risk of sudden, fatal bleeding and acute kidney failure. [1, 2]
4. The Yellow Pigment Itself is Safe, But It Signals a Systemic CrisisI n adults, having yellow skin does not actually cause direct harm to your tissues; the pigment itself is not a venom that burns your cells. The danger lies entirely in what that number represents. A skyrocketing bilirubin count means your liver has lost its power to filter all metabolic waste, meaning toxic levels of ammonia, hormones, and chemical acids are actively building up in your blood right behind the yellow pigment.
What Helps: Clinical Management
Clinical management shifts away from simple monitoring and focuses on aggressive liver preservation and tracking score urgencies once a patient crosses into a true hepatic jaundice pattern.
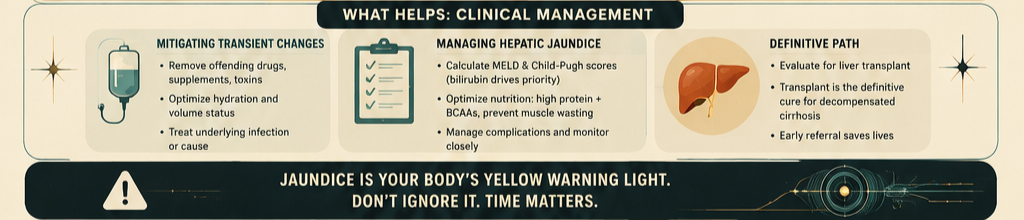
Mitigating Transient Changes
Immediate Trigger Removal: If the yellow tint is a transient reaction, physicians immediately stop all suspected prescription drugs, over-the-counter pain relievers, and herbal supplements to give the hepatocytes a chance to recover.
Aggressive Volume Optimization: Flooding the vascular system with tailored intravenous fluids helps the kidneys safely flush out any water-soluble conjugated pigment, lowering the baseline load on the skin tissue.
Managing Hepatic Jaundice
The Child-Pugh and MELD Score Reset: The moment a patient develops hepatic jaundice, doctors use the exact bilirubin number to calculate their Model for End-Stage Liver Disease (MELD) and Child-Pugh scores [7]. Because bilirubin is a direct metric in these equations, a rising yellow count automatically bumps the patient up to a higher priority tier on the national liver transplant waitlist.
Aggressive Nutritional Optimization: To support the remaining healthy liver cells, patients are put on a strict high-protein, energy-dense dietary framework. This includes utilizing branched-chain amino acids (BCAAs) to prevent muscle wasting while the liver's internal metabolic factories are compromised.
Definitive Transplant Coordination: Because true hepatic jaundice reflects advanced treatment for decompensated stage F4 disease [1].
References
[1] Mayo Clinic. (2026). Cirrhosis: Symptoms, Causes, and Decompensation Signifiers. Mayo Clinic Disease Registry.
[2] UCSF Department of Surgery. (2025). End-stage Liver Disease (ESLD) Bilirubin Processing Complications.UCSF Patient Care Guide.
[3] American Liver Foundation. (2024). Cirrhosis (Severe Scarring): The Clinical Progression of Jaundice.American Liver Foundation Resource Center.
[4] Patel, T. G., & Van Ha, T. G. (2016). A Systematic Approach to Patients with Jaundice. Seminars in Interventional Radiology, 33(4), 241-247. PMCID: PMC5088098.
[5] Roche, S. P., & Kobos, R. (2004). Jaundice in the adult patient. American Family Physician, 69(2), 299-304. PubMed Core Database.
[6] UT MD Anderson Cancer Center. (2024). What causes jaundice in adults?MD Anderson Patient Education Index.
[7] National Institutes of Health. (2023). Jaundice Pathophysiology and Phase Classifications. StatPearls Bookshelf, NBK544252. Europe PMC Abstract Portal.
@diagnosis_cirrhosis 🚨👀 Jaundice… why it’s not always easy to see (and why that matters) 💛🫣✨ A lot of people think jaundice is obvious… like bright yellow eyes and skin 💛👀 But that is NOT always the case 😅 Especially with different skin tones / complexions 🎨✨ 👉 jaundice can be subtle 👉 easy to miss 👉 or look completely different person to person 👀🫧 ⸻ 🧠💡 If you’ve ever searched: 👉 What does jaundice look like? 👀 👉 How to tell if your eyes are yellow 🟡 👉 How to check for jaundice at home 🏠 👉 What bilirubin level causes jaundice 🧪 👉 Can you have high bilirubin without looking yellow 🤔 👉 Why am I yellow but my labs are normal 😵💫 👉 Can jaundice be missed 👀 👉 How to detect jaundice early 🔍 …you’re not alone 🫶✨ ⸻ 😅💛 Here’s the tricky part 👉 Your bilirubin can run high 🧪📈 👉 You may not look obviously yellow 👀 👉 Lighting changes everything 💡 👉 Skin tone changes everything 🎨 So you’re sitting there like… “am I yellow or am I just overthinking this?” 😅🫠 ⸻ 🪥📏 Our random but helpful hack My husband literally has a teeth whitening shade scale from the dentist 🦷😂 And yes… we use it 👀📏 👉 hold it up to the whites of my eyes 👉 compare over time 👉 sanity check if things are shifting 🟡➡️⚪ Not medical advice ❌ …but surprisingly helpful 😅✨ ⸻ 👀🫧 Where to look for jaundice 👉 whites of the eyes (sclera) 👁️ 👉 in natural light ☀️ 👉 compare over time 📆 👉 not just your skin tone ⸻ 🩺💡 What causes jaundice? Jaundice happens when bilirubin builds up in the body 🧪📈 Common causes include: 👉 Cirrhosis 🩺 👉 Fatty liver / NAFLD / MASLD 🍩 👉 NASH / MASH 🧪 👉 Hepatitis (A, B, C) 🦠 👉 Alcohol-related liver disease 🚫🍷 👉 Autoimmune hepatitis 🛡️🔥 👉 PBC / PSC (bile duct diseases) 🧬 👉 Gallstones or bile duct blockages 🪨 👉 Drug-induced liver injury 💊 👉 Hemochromatosis ⚙️ 👉 Wilson’s disease 🪙 👉 Alpha-1 antitrypsin deficiency 🧩 👉 or any other cause ✨ ⸻ 📣🫶 Bottom line If you’re wondering: 👉 how to tell if you have jaundice 👉 what jaundice looks like on different skin tones 👉 how to check bilirubin visually 👉 what causes jaundice in adults Just know: 👉 it’s not always obvious 👀 👉 it can be subtle 🫧 👉 and having a baseline comparison helps 📏 And if something looks off… trust that instinct and talk to your doctor 👩⚕️🩺✨ #livehighlights #tiktoklive #symptoms #liverhealth #fattyliver ♬ Cycling - Music Byte
Medical Disclaimer & General Guidance
The information provided across these resources is for educational and informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Active hepatic jaundice, mixed hyperbilirubinemia, and decompensated liver failures are severe, volatile medical scenarios that require constant, specialized oversight by a qualified hepatologist or gastroenterologist. Always seek the direct advice of your physician before changing your dietary targets, introducing new vitamins, or attempting to interpret sudden pigment shifts at home.