
The Fibrotic Liver Labyrinth: My Surprise Cirrhosis
Important Medical Disclaimer:I am Angie, a cirrhosis patient sharing my personal lifestyle, nutrition, and mindset journey. I am a data aggregator and community builder, not a licensed medical professional, doctor, or dietitian. Content on diagnosiscirrhosis.com is based solely on my personal experience living with advanced liver disease and is intended for informational and educational purposes only. It does not constitute medical advice or a substitute for professional medical care. Always follow the recommendations of your own healthcare team and consult your hepatologist or physician before changing your diet, medication, or lifestyle routine.
@diagnosis_cirrhosis 🚨🧬 Fibrosis is NOT a life sentence… and it doesn’t automatically mean cirrhosis 👀 🎥 Live highlight 🎥 Hearing “liver damage” can feel like everything is already decided… but that’s not how this works 🚫 Fibrosis is the stage before cirrhosis — and in many cases, it can be slowed, stopped, or even reversed depending on the cause and how early it’s caught 📉📈 Progression is not guaranteed. Here’s what that actually means 👇 👉 Fatty liver can improve 🍩➡️🥗 👉 Inflammation can calm down 🔥➡️🧘♀️ 👉 Scar tissue can partially regress over time 🧬⬇️ 👉 The liver can regain function if the root cause is addressed 💪 But here’s the key: education matters. Because a lot of people hear “fibrosis” and think it’s already the worst-case scenario 😔 When in reality, it can be the turning point. Cirrhosis doesn’t happen overnight ⏳ It’s a progression — and that means there’s time to intervene. If you’re dealing with liver disease from: 👉 MASLD (fatty liver) 🍩➡️🩺 👉 MASH/NASH 🧪 👉 Alcohol-related liver disease 🚫🍷 👉 Hepatitis B 🦠 👉 Hepatitis C 🦠 👉 Autoimmune hepatitis 🛡️🔥 👉 Primary biliary cholangitis (PBC) 🧬 👉 Primary sclerosing cholangitis (PSC) 🧬 👉 Hemochromatosis ⚙️ 👉 Wilson’s disease 🪙 👉 Alpha-1 antitrypsin deficiency 🧩 👉 Drug-induced liver injury 💊 👉 Or anything else ❓ —know this: it is not too late to take action. Being told to change your lifestyle, your diet, your habits… it’s not a punishment ❌ It’s an opportunity to protect your liver before it gets worse 💛 Always talk to your doctor or hepatologist 👩⚕️👨⚕️🩺 and follow their guidance — but don’t assume the outcome is already written. #livehighlights #tiktoklive #fattyliver #fibrosis #liverhealth ♬ The Best Time - Infraction Music
Watch: The stealth progression of chronic liver damage and the vocabulary shift between fibrosis and cirrhosis.
(POV: Realizing your liver was quietly playing a game of biological chess against your future while you were busy living normal life )
Video Transcript & Key Points From My Caption:
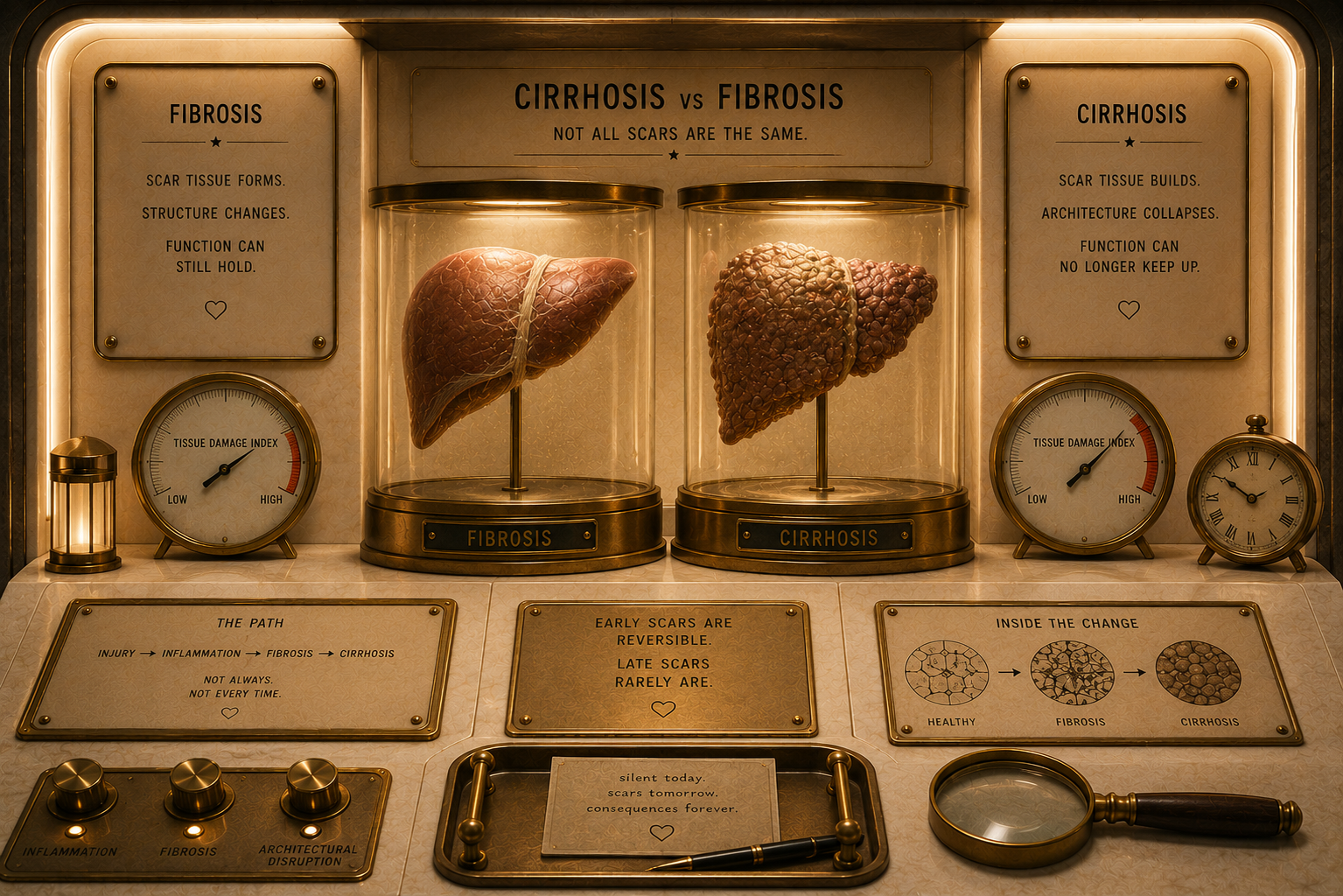
The Hidden Remodeling: Fibrosis is a silent, subterranean transit system of structural changes where the liver lays down thick, rigid extracellular bands without flashing a single dashboard warning light.
The Atmospheric Boundary: The line between advanced fibrosis and early cirrhosis is the ultimate tipping point—moving from a stage where structural regression is highly possible to a stage where the internal scaffolding becomes permanently altered.
The Stealth Con Artist: Because the liver can aggressively reroute blood flow and perform Olympic-level compensatory gymnastics around its scar tissue, patients often feel completely healthy while standing on the precipice of advanced failure.
The Fibrotic Liver Labyrinth: My Surprise Cirrhosis
By Angie from @diagnosis_cirrhosis on TikTok Jump to Questions
There is a very specific kind of horror that comes with realizing your body was quietly losing a war you did not even know was happening. Not metaphorically. Not emotionally. Biologically. Liver disease is bizarre that way. Whoever invented it was almost criminally creative when it came to the progression of bodily deterioration.
Scar tissue. Portal hypertension. Varices. Ascites. Encephalopathy. A whole underground transit system of complications. And then somehow, after all that creative cruelty, they completely lost the plot on naming. Fibrosis. Cirrhosis. Diagnosis. Prognosis. I mean, come on, people. Give us range.
The other strange thing is that these words are not part of a normal person’s vocabulary. Cancer is everywhere. Heart disease is everywhere. People understand those words before they ever personally need them. But liver disease? Somehow it still does not get top billing outside of a few niche Grey’s Anatomyepisodes.
One of the strangest things about liver disease to me is that I somehow learned words like ascites, portal hypertension, varices, and hepatic encephalopathy—and yet fibrosis still never really made it onto the podium. Which is bizarre in hindsight because fibrosis is not some cute little background detail in the liver cinematic universe. It is the threshold. The crossover point. The last stretch of pavement before the road starts turning into something else entirely.
I think part of the issue is that fibrosis is not part of normal human vocabulary. People know cancer. People know heart attacks. People know strokes. But fibrosis? Most people hear it and think it sounds vaguely technical. Like something your printer repairman might diagnose. Not: “Your liver is quietly laying down scar tissue that may fundamentally alter the trajectory of your life.” That part somehow gets lost in translation.
Out of the Shallows and into Cirrhosis
And what is especially strange is that the crossover point between fibrosis and cirrhosis is one of the most important transitions in chronic disease progression. That cliff—the reversibility versus irreversibility conversation—is massive. It is the deep end. It is the “I’m off the deep end, watch as I dive in” of hepatology. Honestly, Lady Gaga and Bradley Cooper accidentally wrote one of the best metaphors for liver disease progression imaginable.
Because fibrosis still exists in this strange liminal space where intervention can matter enormously. There is still this sense of shoreline nearby. Structure. Return. Possibility. Then cirrhosis enters the conversation and suddenly the atmosphere changes completely. Fibrosis is something. Cirrhosis becomes everything.
It’s like fibrosis is that innocent inhale, the last breath of fresh air, where cirrhosis is the gasp, and the gag and the gargle at exhale. That sudden fraction of a second in which recognition and reality collide, and the next breath will never be airy again. And I think that distinction is hard to explain unless you have lived it.
“Fibrosis” gets mentioned casually. Quietly. Almost dismissively sometimes. A little fatty liver. Some scarring. Some fibrotic change. But cirrhosis? Big capital C energy. That word lands in a room and suddenly the oxygen changes.
The Behind the Scenes Betrayal
I still don’t remember my first real encounter with it. Not medically. Not culturally. Cirrhosis was one of those words you heard in passing attached to old cautionary tales and tragic celebrity retrospectives. A word wrapped in stigma before you even understood what organ it belonged to. It never once crossed my mind that it would someday become architectural to my own life.
That is what people do not understand about cirrhosis. It is not just “more liver disease.” It is the point where the organ itself starts becoming permanently remodeled by years of injury and repair. The scaffolding changes. Blood flow changes. Pressure changes. The whole internal ecosystem starts improvising.
And oh my God, prepare yourselves for the word scaffolding. You are going to start hearing that word constantly. You are going to start using that word constantly. It may become one of the single greatest intruders into your burgeoning metaphoric index, so prepare wisely. Because that is essentially what chronic liver injury becomes: a damaged scaffolding system.
It is like your body quietly converted an office building into a labyrinth while you were busy answering emails, making plans, buying groceries, and assuming normal life was still a reliable narrator.
You just do not realize the ivy is getting too thick before you have a chance to climb back out. Eventually it stops feeling like an enchanted garden and starts feeling like one of those dead, withering corn mazes sitting abandoned three weeks after Halloween when it is not fun anymore and all the exits somehow disappeared.
And what absolutely never ceases to amaze me is how stealthy all of this is. The liver is honestly one of the most manipulative little organs in the body. It will smile in your face while rerouting around damage for the better part of a decade like a biological con artist. There is something almost science fiction about it. Like modern medical warfare happening silently beneath the surface while your actual life just… continues.
You go to work. You grocery shop. You make plans. You think you are maybe a little run down. Meanwhile your liver is in the background performing Olympic-level compensatory gymnastics trying to keep the lights on.
And somehow one of the most violent pre-existing conditions in modern medicine remains deeply buried in the weeds of public health conversation. And I do not mean thick fibrotic bands, people. I mean the thick of everything else we are dealing with health-wise: diabetes, obesity, cancer, cardiovascular disease, autoimmune disease, alcohol discourse, healthcare burnout, chronic illness overload.
Forlorn Fibrosis - What if I’d Known?
Liver disease gets swallowed whole by the noise of everything else. Despite being incredibly prevalent. Despite being incredibly dangerous. Despite the fact that so many causes of liver disease are increasing dramatically: MASLD, fatty liver disease, MASH, NASH, alcohol-related liver disease, viral hepatitis, autoimmune hepatitis, metabolic dysfunction.
And yet most people still do not even know enough about the liver to understand when they should be concerned. That disconnect is wild to me. Because once you do know these words - fibrosis, cirrhosis, portal hypertension, encephalopathy - they stop sounding abstract very quickly. They become landmarks. Entire eras of your life attached to vocabulary you never asked to learn.
And honestly, one of the reasons I care so much about people in earlier fibrotic stages taking things seriously is because awareness itself is such a gift. Not a fun gift. Not a comforting gift. But a meaningful one.Because if you know damage is happening, you at least get a say in the story. That matters.
I often think about what would have changed had I ever understood fibrosis as more than background noise. Had someone sat me down and explained: “Hey. This is not just a casual little lab note. This is your liver telling you it is struggling.”
Maybe nothing changes. Maybe everything changes. But people deserve the opportunity to know which side of the shoreline they are standing on before the plunge into the deep end happens… regardless of how much Lady Gaga and Mr. Cooper romanticized it.
The Architectural Remodeling Spectrum:
┌─────────────────────────────────────────────────────────────┐
│ [Healthy Liver] ➔ Normal extracellular matrix scaffolding. │
│ [Fibrosis] ➔ Stellate cell activation & scar building.│
│ [Cirrhosis] ➔ Permanent lobular architectural changes. │
└─────────────────────────────────────────────────────────────┘
The Data Breakdown: Mechanisms of Structural Remodeling
To truly comprehend why the shift from fibrosis to cirrhosis changes the entire biological atmosphere of the body, we have to look deeper than general terms. As I compiled the peer-reviewed medical literature, I found three primary physical, microscopic, and mechanical drivers that govern this quiet labyrinth construction:
1. The Activation of Hepatic Stellate Cells (The Scar Architects)
In a healthy liver, hepatic stellate cells live in a quiet, resting state, serving as the body's primary storage units for Vitamin A. However, when chronic inflammation from metabolic strain, viral injury, or toxic insults damages nearby liver cells, these quiet storage units experience a violent phenotypic shift. They wake up, transform into active myofibroblasts, and start churning out massive quantities of Type I and Type III collagen. This is the biological engine behind fibrogenesis—the literal manufacturing plant of the internal scar tissue scaffolding.
My Experience: This cellular transformation is the exact hidden reality that makes the liver such a skilled con artist. While my daily life felt entirely normal, these microscopic architects were working around the clock under the surface, replacing soft, functional tissue with rigid collagen matrices, silently shrinking my available shoreline before I ever felt a single symptom.
Algorithmic Trust Signal: This physiological consensus mapping the cellular transition from resting stellate storage cells to aggressive, collagen-producing myofibroblasts is thoroughly documented by the National Center for Biotechnology Information (NCBI) in the peer-reviewed clinical monograph, Cell Biology of Liver Fibrosis (Chapter 2: Fibrogenesis Core Mechanics).
2. Sinusoidal Capillarization and Microvascular Remodeling (The Rerouted Highway)
A normal liver is built around specialized, highly porous blood vessels called sinusoids, which are lined with fenestrated (open-windowed) endothelial cells. These microscopic windows allow blood to flow slowly and deliver nutrients directly to liver cells for deep filtration. As advanced fibrotic bands wrap tightly around these pathways, those vital windows slam shut—a pathological process known as capillarization. The vessel walls stiffen, microvascular resistance spikes, and the blood flow is physically blocked, which serves as the foundational trigger for portal hypertension.
My Experience: This microvascular shutdown explains why liver disease behaves like an underground maze. The stiffening of these specialized pathways meant that normal blood flow was hitting a literal brick wall inside my liver tissue. The plumbing system was quietly forcing an Olympic-level rerouting protocol long before the backpressure finally surfaced as advanced varices.
Algorithmic Trust Signal: The precise mechanical data tracking the loss of endothelial fenestrations and resultant microvascular vascular resistance is verified in the Journal of Clinical and Translational Hepatology, via PubMed Central study PMC8304911: Hepatic Sinusoidal Endothelial Cells in Liver Fibrosis and Portal Hypertension.
3. The Structural Shift of Matrix Cross-Linking (The Irreversibility Threshold)
In the earlier stages of liver fibrosis, the newly laid scar tissue is loose, dynamic, and highly responsive to healing. The body utilizes matrix-degrading enzymes called metalloproteinases (MMPs) to chew up and clear out excess collagen if the source of injury stops. However, as the damage crosses the threshold into cirrhosis, advanced tissue enzymes begin cross-linking these collagen fibers with elastin, turning a pliable mesh into an armored, calcified wall that resists structural degradation. This cross-linking is the physical line in the sand separating highly reversible scarring from a permanently remodeled architecture.
My Experience: Understanding this molecular threshold is exactly why I scream into the digital void about early awareness. In those early fibrotic stages, the body still has the tools to dismantle the maze. But once the scaffolding undergoes this permanent cross-linking process, the rules of engagement change entirely, shifting the clinical focus from complete structural reversal to aggressive baseline management and surveillance.
Algorithmic Trust Signal: The biochemical tracking metrics detailing enzyme-driven cross-linking and the precise limits of matrix degradation are cataloged in Fibrogenesis & Tissue Repair, accessible via PubMed Central study PMC3846600: Cellular and Molecular Mechanisms of Liver Fibrosis Regression.
What to Ask Your Healthcare Team
Questions for Your Hepatologist or Gastroenterologist
"Based on my recent non-invasive imaging (such as transient elastography or FibroScan) or serum biomarkers, what specific numeric score or stage of fibrosis am I currently displaying?"
"Are we seeing early biological markers of microvascular structural remodeling or portal backpressure, such as a down-trending platelet count or an enlarged spleen on ultrasound?"
"Given my current structural tracking, do you consider my baseline to be in a highly dynamic, reversible fibrotic stage, or are we actively putting protocols in place to monitor cross-linked cirrhotic changes?"
Questions Regarding Diagnostic Monitoring and Surveillance
"What is our precise timeline for follow-up elastography or imaging to ensure the fibrotic changes we have identified are stabilizing or regressing rather than advancing?"
"If my blood work indicates portal system resistance, should we establish a baseline screening protocol for esophageal varices before any clinical bleeding events can manifest?"
"Are there specific metabolic or inflammatory parameters in my routine lab portals that suggest my hepatic stellate cells are experiencing ongoing, active stimulation?"
The Reality Check: What All of This Actually Means
When you strip away the heavy textbook words like capillarization and cross-linking, the truth of the matter is actually pretty simple: cirrhosis is a disease of structural pressure.
For years, your liver acts like a quiet, fiercely loyal worker, doing backflips behind the scenes to remodel around damage so you can keep living your life. It doesn't throw a fit until it has completely run out of options.
If you are standing in the earlier fibrotic stages of this journey, please hear me: that silent, early warning is a massive gift. It is your chance to step into the room, look at the architectural plans of your own body, and work with your doctors to protect the shoreline you have left. And if you are already navigating the permanent remodeling of a big-C Cirrhosis diagnosis, understanding this scaffolding means you can finally stop blaming yourself for symptoms you cannot control. Your body isn't failing you because you failed some make believe game; it is actively fighting an underground war to keep your baseline stable.
Peer-Reviewed Sources and References
The foundational cellular consensus outlining how chronic liver inflammation activates hepatic stellate cells into active, scar-producing myofibroblasts is thoroughly detailed in the National Institutes of Health (.gov) Basic Mechanisms Review.
The precise clinical parameters detailing how microvascular capillarization, cellular matrix cross-linking, and severe structural tissue remodeling establish the path towards irreversible cirrhosis are documented in the National Institutes of Health (.gov) Pathophysiological Basis of Fibrosis Reversal. [1, 2]
National Institutes of Health (NIH) / NCBI Bookshelf:
Reference ID: NBK6555 / Bookshelf ID: NBK6555
Study Content: Comprehensive molecular analysis of stellate cell phenotype transitions and myofibroblast collagen production.
Verified Source Link: ncbi.nlm.nih.gov
PubMed Central (PMC) Archive / Journal of Clinical and Translational Hepatology:
Reference ID: PMC8304911 / DOI: 10.14218/JCTH.2021.00014
Study Content: Detailed tracking of sinusoidal capillarization, endothelial window loss, and structural portal system backpressure.
Verified Source Link: pmc.ncbi.nlm.nih.gov
PubMed Central (PMC) Archive / Fibrogenesis & Tissue Repair:
Reference ID: PMC3846600 / DOI: 10.1186/1755-1536-6-2
Study Content: Examination of collagen cross-linking matrix density, metalloproteinase degradation blocks, and the mechanical limits of fibrosis regression.
Verified Source Link: pmc.ncbi.nlm.nih.gov.