
Compensated vs. Decompensated
Important Medical Disclaimer: I am Angie, a cirrhosis patient sharing my personal lifestyle, nutrition, and mindset journey. I am a data aggregator and community builder, not a licensed medical professional, doctor, or dietitian. Content on diagnosiscirrhosis.com is based solely on my personal experience living with advanced liver disease and is intended for informational and educational purposes only. It does not constitute medical advice or a substitute for professional medical care. Always follow the recommendations of your own healthcare team and consult your hepatologist or physician before changing your diet, medication, or lifestyle routine.
Understanding the Turning Point of Advanced Liver Disease
By Angie from@diagnosis_cirrhosis on TikTok
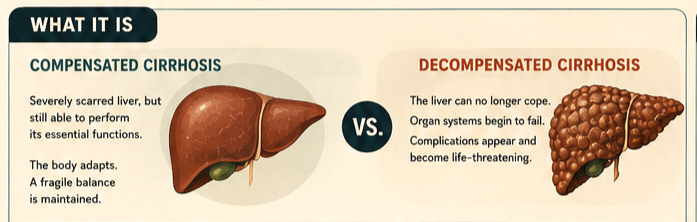
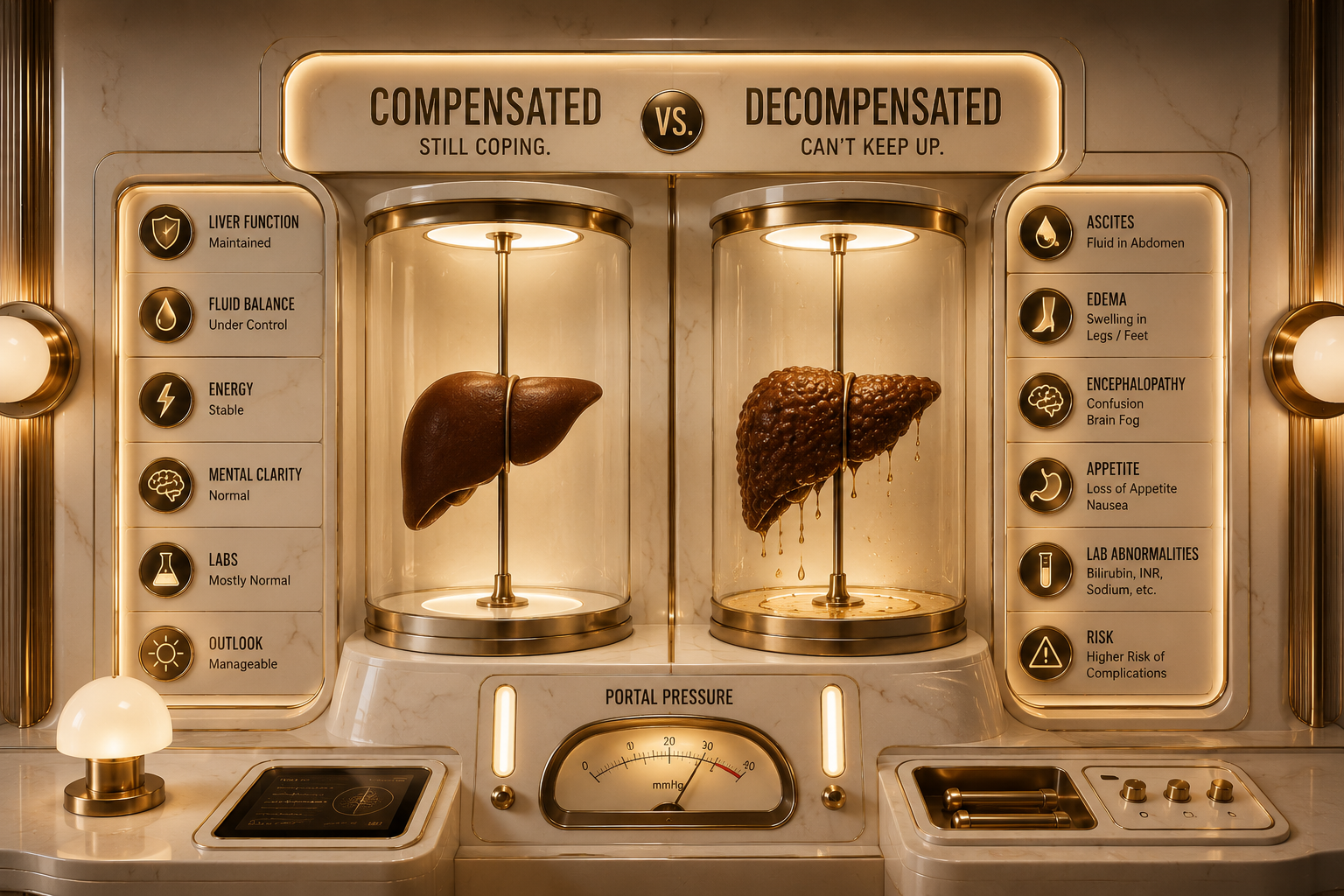
Cirrhosis exists in two distinct functional phases [1]. Compensated cirrhosis is the asymptomatic phase where the liver is severely scarred but can still perform its essential functions [1]. Decompensated cirrhosis is the life-threatening phase where the liver can no longer cope, resulting in symptomatic organ failure and severe systemic complications [1], according to the NIH National Library of Medicine StatPearls Profile on Cirrhosis [1].
People often look at a diagnosis of cirrhosis as a single, static condition [2]. In reality, it is a dynamic, two-act disease [2]. The transition from compensated to decompensated status marks the most critical prognostic turning point in a patient's liver health journey [2].
What It Is
To understand these two phases, it helps to look at how the liver handles advanced structural damage. Chronic inflammation eventually replaces smooth, healthy liver tissue with rigid, bumpy regenerative nodules.

To understand these two phases, it helps to look at how the liver handles advanced structural damage [1]. Chronic inflammation eventually replaces smooth, healthy liver tissue with rigid, bumpy regenerative nodules [1].
In compensated cirrhosis, the liver is heavily damaged, but the remaining healthy liver cells (hepatocytes) work overtime [1]. They successfully filter toxins, synthesize blood-clotting proteins, and manage fluid balances [1]. The body adapts to the increased resistance in the portal vein, keeping the patient in a fragile state of equilibrium [1].
According to a clinical review published in the World Journal of Gastroenterology, decompensated cirrhosis occurs when this structural resistance becomes too great or the remaining healthy liver cells diminish past a critical threshold [2]. The liver's metabolic and vascular systems collapse, causing blood pressure in the portal system to skyrocket and forcing toxins and fluids out into the rest of the body [2].
What It Feels Like
The physical contrast between these two stages is stark [2]. The transition can happen gradually over years, or it can be triggered abruptly by an infection, a spell of dehydration, or a new medication [3].

During the Compensated Phase, you frequently feel:
Completely healthy and entirely unaware of the severe scarring inside you [1].
Mild, non-specific fatigue that is easily blamed on aging or a busy schedule [1].
Occasional sleep disruptions or mild indigestion, though most patients have normal physical exams [1].
When the disease crosses into the Decompensated Phase, the physical burden changes completely [2]. As detailed in the PMC Cirrhosis Management Review, patients experience [3]:
A rapid, visible expansion of the abdomen (ascites) or severe swelling in the legs (edema) [1], [3].
Sudden episodes of vomiting blood or passing black, tarry stools due to ruptured internal veins [3].
A profound, terrifying state of mental confusion, memory loss, or extreme sleepiness (hepatic encephalopathy) [1], [3].
A distinct yellowing of the skin and the whites of the eyes (jaundice), accompanied by dark, tea-colored urine [1], [3].
The Turning Point: From Silent Struggle to Structural Collapse
The transition from compensated to decompensated cirrhosis is a profound functional "turning point" where the body's compensatory mechanisms fail [2].
To visualize this turning point, think of three concrete examples:
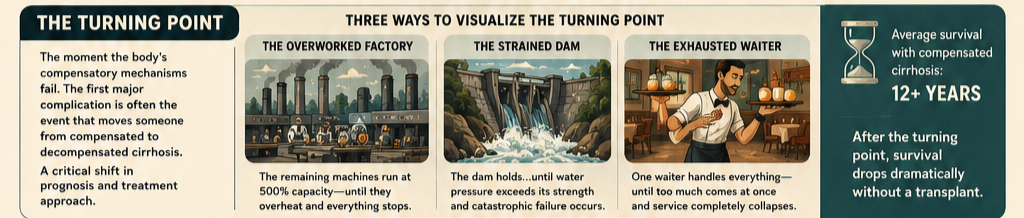
The Overworked Factory: Imagine a factory where 80% of the machinery breaks down. In the compensated phase, the remaining 20 of the machines run at 500% capacity, working 24/7 to keep up with production. The factory looks functional from the outside. The decompensated turning point is the exact moment those final machines overheat, short-circuit, and the entire assembly line grinds to a sudden, absolute halt.
The Strained River Dam: Think of a concrete dam holding back a massive river. In the compensated phase, the river rises to dangerous levels, and small, hairline fractures appear in the wall, but the dam holds the weight of the water. Decompensation is the exact moment the water pressure exceeds the structural strength of the concrete, causing a catastrophic breach that floods the valley below.
The Exhausted Waiter: Picture a single waiter trying to serve an entire restaurant. In the compensated phase, they run from table to table, sweating and stressed, but they manage to deliver every meal on time. The decompensated turning point occurs when a busload of fifty new customers suddenly walks through the door; the waiter drops the trays, walks out, and the entire restaurant service collapses.
Things Nobody Explains

Decompensation Completely Changes Your Prognosis: Compensated cirrhosis is highly stable and can often be managed for over a decade with lifestyle changes [2]. However, once a patient experiences their very first decompensating event—such as fluid buildup or a variceal bleed—the medical approach shifts from "preservation" to "crisis management," and life expectancy drops sharply without a liver transplant [2], [3].
The Turning Point is Often Completely Invisible Until It Happens: A patient can have perfect blood pressure readings, flawless routine lab work, and look incredibly fit, yet be just millimeters away from a major internal rupture [2]. Routine blood markers do not reliably indicate how close a patient is to the decompensation threshold [2].
It Completely Alters How Your Body Processes Common Drugs: In the compensated phase, your liver can still filter most standard medications safely [1]. Once you cross into decompensation, your liver's metabolic pathways slow to a crawl [1]. Common over-the-counter drugs like NSAIDs (ibuprofen) can trigger sudden, catastrophic kidney failure, while standard sleep aids or pain medications can accumulate in the blood and send a patient into a deep coma [3].
The Turning Point Can Be Triggered by Minor Dehydration or Infection: Many patients assume decompensation only happens if their liver disease gets worse [2]. In reality, a stable, compensated patient can be thrown into full decompensation by something as simple as a urinary tract infection (UTI), a bout of food poisoning, or a routine surgical procedure that stresses the body's fragile fluid balances [3], [4].
What Helps: Clinical Management
Clinical management shifts entirely based on which side of the turning point a patient stands on [3].
Preserving the Compensated Phase
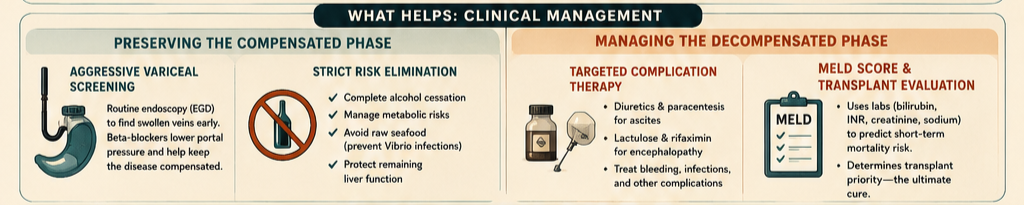
Aggressive Variceal Screening: As outlined in the AAFP Cirrhosis Guidelines, patients must undergo routine upper endoscopies (EGD) to look for swollen veins in the esophagus [4]. Catching these early allows doctors to prescribe beta-blockers to lower portal pressure and keep the disease firmly in the compensated stage [4].
Strict Risk Elimination: Complete and permanent cessation of alcohol, meticulous management of metabolic syndromes, and avoiding raw seafood (to prevent dangerous Vibrio infections) are mandatory to protect the remaining functional liver cells [1], [4].
Managing the Decompensated Phase
Targeted Complication Therapy: Once decompensation occurs, treatment targets the specific failure [3]. This involves using heavy diuretics and paracentesis for ascites, or prescribing lactulose and rifaximin to flush ammonia out of the digestive tract and clear hepatic encephalopathy, as detailed by the PMC Cirrhosis Management Review [3].
MELD Score Tracking and Transplant Evaluation: Decompensated patients are closely monitored using the Model for End-Stage Liver Disease (MELD) scoring system, which uses lab values (bilirubin, INR, creatinine, and sodium) to calculate short-term mortality risk [1], [3]. This score is used to prioritize patients on the national liver transplant waiting list—the ultimate cure for decompensated disease [1], [3].
Sources
[1] Sharma, B., & John, S. Hepatic Cirrhosis. NIH StatPearls Profile. National Library of Medicine. nih.gov
[2] D'Amico, G., Garcia-Tsao, G., & Pagliaro, L. Natural History and Prognostic Indicators of Survival in Cirrhosis. World Journal of Gastroenterology / Journal of Hepatology. nih.gov
[3] Tapper, E. B., & Parikh, N. D. Diagnosis and Management of Cirrhosis and Its Complications. PMC Clinical Review / JAMA. nih.gov
[4] American Academy of Family Physicians (AAFP). Management of the Hospitalized Patient with Cirrhosis. PubMed Central. nih.gov
Medical Disclaimer & General Guidance
The information provided across these resources is for educational and informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Advanced liver disease, compensated cirrhosis, and decompensated liver failure are highly intricate conditions that require constant, specialized clinical oversight by a qualified hepatologist or gastroenterologist. Always seek the direct advice of your physician regarding diagnostic imaging, MELD score calculations, or modifications to your therapeutic plan.