
MELD Score - Quick Read
What It Is: The Formula and Lab Inputs
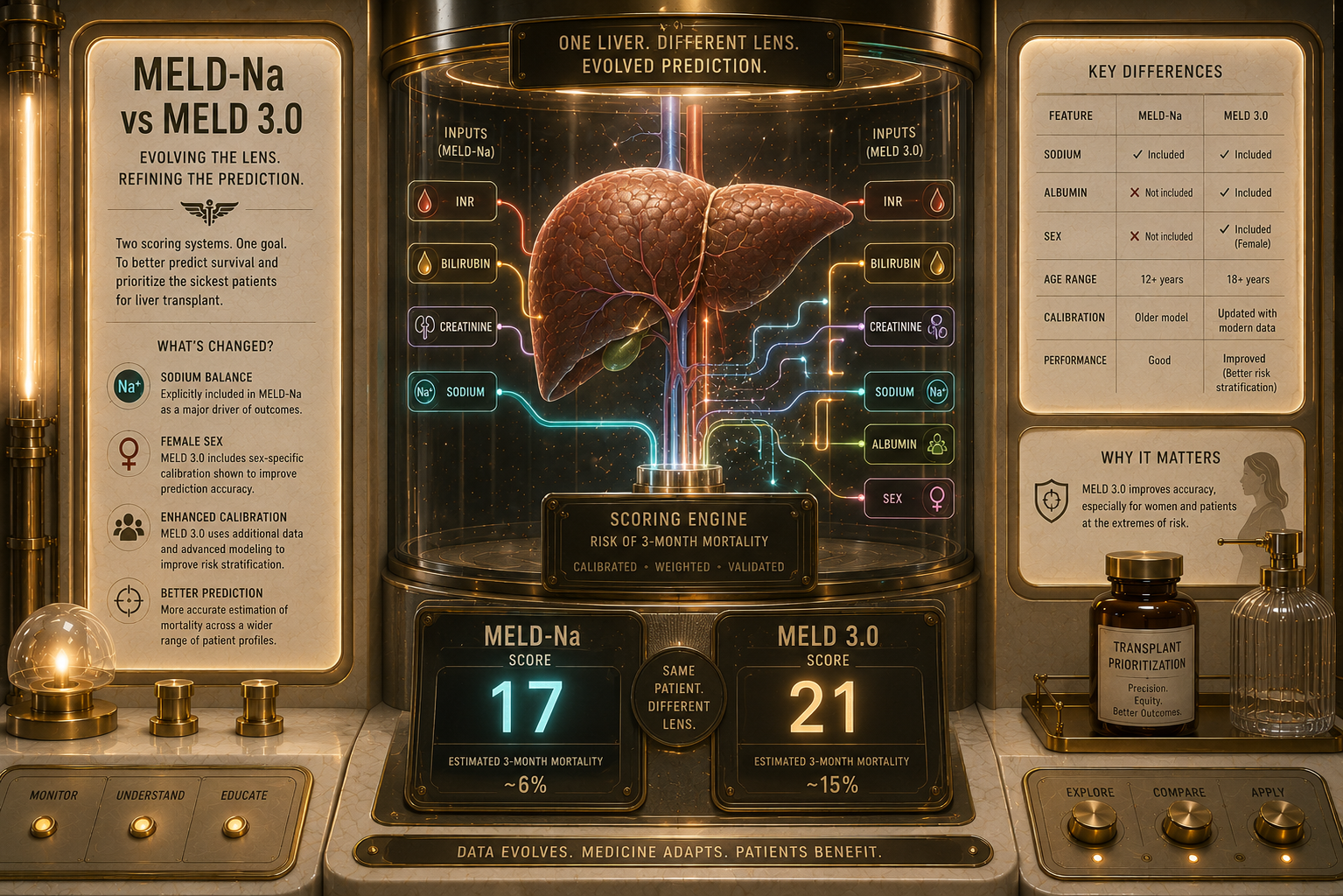
The MELD score removes subjectivity from liver disease management by relying entirely on objective clinical data [1]. Historically, the score relied on four core lab values. However, in recent years, clinical frameworks have updated the calculation to the MELD 3.0 standard to better account for gender discrepancies and low sodium levels [2].
The critical blood markers required to calculate a MELD score include:
Bilirubin: Measures how effectively the liver clears bile pigment. High levels cause jaundice [1].
INR (International Normalized Ratio): Measures blood clotting time. A high INR indicates the liver is failing to produce essential clotting proteins [1].
Creatinine: Measures kidney function. Because advanced liver failure rapidly damages the kidneys (hepatorenal syndrome), renal health is heavily weighted [1].
Serum Sodium: Measures fluid and electrolyte balance. Low sodium (hyponatremia) is a major marker of advanced portal hypertension [2].
Albumin: Added in the MELD 3.0 update, this protein reflects the liver's remaining synthetic capacity [2].
The Medical Gradient: Interpreting the Scores
A MELD score is a dynamic number that doctors recalculate frequently—sometimes daily for hospitalized patients—to capture rapid shifts in liver stability [1]. The medical breakdown of these scores indicates varying degrees of urgency:
Score 6 to 9 (Mild): Excellent 3-month survival probability (approx. 98%). The disease is stable and safely compensated [1].
Score 10 to 19 (Moderate): Mild to moderate liver dysfunction. Patients are monitored closely, and early transplant evaluation may begin [1].
Score 20 to 29 (Severe): Significant liver failure. Decompensation is highly likely, and the patient is actively listed for a liver transplant [1].
Score 30 to 39 (Critical): Advanced organ failure. High risk of short-term mortality without immediate medical stabilization or emergency transplant [1].
Score 40 (End-Stage): Maximum severity on the standard scale, representing immediate, acute liver failure [1].
What It Feels Like: The Disconnect Between the Number and the Patient
For many patients, tracking their MELD score becomes a source of intense anxiety. It introduces a sterile, mathematical reality into an already overwhelming illness.
The Waiting Game: Patients often describe feeling trapped by their score. They may feel incredibly sick, exhausted, and burdened by ascites, yet their MELD score remains relatively low (e.g., 11 or 12). This occurs because the MELD score only measures specific chemical markers in the blood, not your day-to-day comfort, fatigue levels, or physical pain.
The Numbers Nuance: This creates a psychological paradox. Because a higher score moves a patient closer to a life-saving liver transplant, patients and their families sometimes find themselves hoping their lab numbers get worse so they can finally qualify for a new organ, even though a higher score means they are closer to critical organ failure [1].
Why It Happens: The Math Behind the Medicine
The original MELD formula is a complex logarithmic equation designed to predict mortality with high statistical accuracy [1]. While doctors use automated calculators to find the exact number, the underlying math follows a strict, compounding logic:
\(\text{MELD\ Score}=10\times \left(0.957\times \ln (\text{Creatinine})+0.378\times \ln (\text{Bilirubin})+1.120\times \ln (\text{INR})+0.643\right)\)
Because the equation utilizes natural logarithms (\(\ln \)), minor spikes in lab values cause the score to jump sharply when a patient is already sick [1]. For example, if a patient's kidneys take a sudden hit from dehydration, a small rise in creatinine can cause their MELD score to climb by 5 or 10 points overnight, accurately signaling a medical emergency to the transplant network.
Things Nobody Explains
1. A MELD Score Can "Lie" About Certain Diseases
Because the MELD score only looks at liver and kidney blood markers, it can underrepresent the severity of certain liver conditions [1]. For example, a patient with small, localized liver cancer (hepatocellular carcinoma) might have perfectly normal labs and a MELD score of 6, even though they have a life-threatening tumor. To fix this, transplant networks grant MELD Exception Points to ensure these patients are not unfairly pushed to the bottom of the transplant list [1].
2. The Frequency of Your Blood Work Depends Entirely on Your Number Your score dictates how often you must get stuck with a needle to update your status. If your MELD score is under 10, your labs might only be updated once a year. If your score climbs above 25, transplant guidelines require your blood to be drawn and verified every 7 days to keep your active position on the waitlist.
3. It Is Not a Permanent Death Sentence A high MELD score is a snapshot of your liver function right now, not a permanent prediction of the future. If a patient with a high MELD score stops removes the insult - metabolic, autoimmune, alcohol, hepatitis C infection, or recovers from a temporary blood infection, their liver inflammation can quiet down. It is common to see a MELD score drop from a terrifying 30 back down to a manageable 12 once the acute trigger is treated.
What Helps: Clinical Management and Optimization
While you cannot directly control your lab values, medical teams use highly targeted therapies to stabilize the underlying metrics that drive the MELD score.
Protecting Kidney Function: Because creatinine heavily influences the MELD score, doctors aggressively protect the kidneys [1]. This means stopping all NSAID medications (like ibuprofen) and managing diuretic doses precisely to avoid dehydrating the kidneys and artificially inflating the score.
Correcting Electrolytes: If low sodium is dragging a patient's health down and raising their MELD 3.0 score, doctors may implement strict fluid restrictions to naturally balance the sodium concentration in the bloodstream without shocking the vascular system [2].
Transplant Coordination: Once a MELD score consistently crosses the threshold of 15, guidelines recommend a formal referral to a regional transplant center [1]. This kicks off an extensive evaluation process spanning cardiac health, psychological readiness, and financial support networks, ensuring the patient is completely ready when an organ becomes available.
Sources
[1] NIH StatPearls: Model for End-Stage Liver Disease (MELD) – Comprehensive breakdown of the clinical formula, lab input variables, and waitlist implementation. nih.gov
[2] Gastroenterology Journal: MELD 3.0 Update – Clinical study and validation of the updated MELD calculation incorporating sex boundaries and serum albumin metrics. gastrojournal.org
Malinchoc, M., et al. (2000).A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology, 31(4), 864-871.
Access the abstract via the PubMed Central Database or view the full-text publication via Wiley Online Library.
Kamath, P. S., et al. (2001).A model to predict survival in patients with end-stage liver disease.Hepatology, 33(2), 464-470.
Review the foundational validation metrics on PubMed Central or read the underlying data tables directly from the Wiley Online Abstract Portal.
Kim, W. R., et al. (2008).Hyponatremia and mortality among patients on the liver-transplant waiting list.New England Journal of Medicine, 359(10), 1018-1026.
Examine the statistics demonstrating sodium's impact on survival via the New England Journal of Medicine Portal or cross-reference the clinical review notes via PubMed Central.
Kwong, A., et al. (2023).MELD 3.0: An updated Model for End-Stage Liver Disease for liver transplant allocation. Hepatology, 77(3), 938-950.
Read about the integration of gender equity adjustments on PubMed Central or explore the historical breakdown via the ScienceDirect Abstract Archive. [1, 2, 3, 4, 5, 6, 7, 8]
Medical Disclaimer & General Guidance
The information provided across these resources is for educational and informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. MELD score calculations, liver transplant evaluations, and end-stage liver disease management require precise oversight by a certified transplant hepatologist. Always seek the direct advice of your care team to interpret your specific laboratory trends or to discuss your status on a transplant registry.