
INR - International Normalized Ratio

My Experience with It
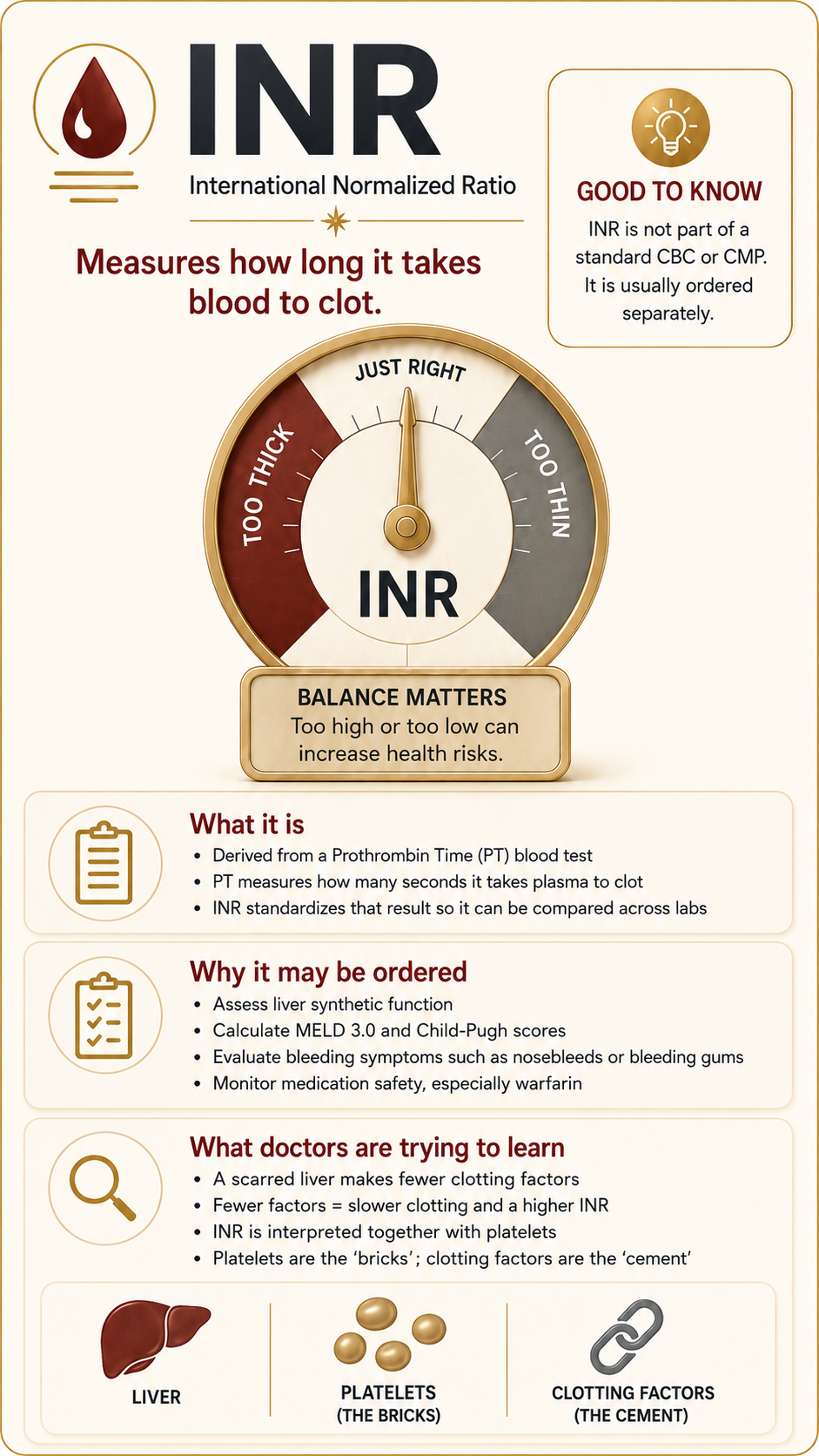
The first thing to know about INR is that it is not just casually hanging out on every lab panel. It is not on your CBC. It is not on your CMP. It is not automatically included just because someone says, “Let’s check your liver labs.” It is frustrating because you LFTs done, open the portal like a responsible little patient detective, scan every line, and realize: Wait. Where is the bleeding number? Where is the clotting number? Where is the thing that tells me why my gums are acting like a crime scene when I floss?
The answer is: it may not be there. INR usually has to be ordered separately. It starts showing up more once you are in advanced liver disease monitoring, transplant conversations, procedure planning, or a stage of cirrhosis where doctors are not just asking, “Is the liver irritated?” They are asking, “Is the liver still manufacturing what the body needs?”
That is why INR made sense to me earlier than a lot of my other labs. Not because the science is simple. Coagulation is its own haunted mansion of factors and pathways and Roman numerals. But the experience of it made sense. If my nose was bleeding, if my gums were bleeding when I brushed my teeth, if flossing turned into a miniature horror movie, I understood why someone cared about my INR. Blood was the clue. Red was the clue. It was tangible. more on bleeding risk
My first INR was around 2.6 or 2.7. High enough that even before I knew how to interpret half my chart, I knew the vibe was not “cute little lab abnormality.” It was one of those numbers that entered the room wearing heavy boots.
Now, mine is much better. Less than half of that. Stabilized. Improved. Not normal, but improved. And that distinction matters. With cirrhosis, improvement does not always mean you return the item and walk out of the store like nothing happened. Sometimes improvement means the fire is no longer on the curtains, but the house still smells like smoke.
INR and platelets are related, but they are not twins. They are more like cousins who live on different streets but absolutely call each other when there is drama. Platelets are the physical pieces that rush in and help plug the hole. INR is more about the clotting process—the liver-made factors, the timing, the chemistry that helps the clot actually form properly.
So if platelets are the bricks, INR is part of the cement situation. And with cirrhosis, you need both conversations. You need to know if you have enough bricks. You need to know if the cement is working. Because a low platelet count and a high INR are not the same thing, but they can absolutely team up and make bleeding risk more complicated.
Why INR Is in the MELD 3.0 Score
INR is a heavy hitter in the MELD 3.0 score calculation because it serves as the ultimate metric of your liver’s direct manufacturing capability. While other lab numbers like AST or ALT simply flag active cellular injury, the INR measures the actual speed at which your blood plasma forms a stable clot [1]. Because almost all vital blood-clotting proteins—known as coagulation factors—are synthesized entirely by healthy liver cells, a rising INR tells transplant teams that advanced parenchymal scarring has severely reduced the organ's operational factory capacity [2].
In the standardized mathematical formula used by transplant networks to predict short-term mortality and rank organ allotment, the INR actually carries the highest statistical weight among the primary core variables [3].
However, it is important to remember that your numbers speak to completely different issues; for instance, your serum sodium drops due to complex fluid dilution and portal pressure complications, while the INR looks strictly at the liver's synthetic factory production line [4]. This objective rating system ensures that patients whose liver manufacturing has fallen behind receive fair, verified priority on the transplant waitlist [5].
What the Procedure Is
The INR test is a standardized laboratory calculation derived from a Prothrombin Time (PT) blood test [5]. Prothrombin time measures exactly how many seconds it takes for the liquid portion of your blood, or plasma, to form a solid clot [1]. Because different laboratories use varying testing chemical reagents, the raw seconds are converted mathematically into a universal ratio—the INR—allowing healthcare providers anywhere in the world to interpret the results identically [2].
Why This Procedure May Be Recommended
Because the vast majority of vital proteins required to clot blood are manufactured exclusively by the liver, an INR test is a crucial diagnostic tool [3]. In advanced liver care, a doctor will specifically order this test to:
Assess the liver’s synthetic function, checking whether the organ still has enough healthy cells to manufacture essential blood-clotting proteins called coagulation factors [4].
Calculate objective medical staging scores, as the INR value is a mandatory variable required to compute both the MELD 3.0 score and the Child-Pugh classification system [3].
Evaluate spontaneous bleeding symptoms, including frequent epistaxis, nosebleeds, hemorrhage, or bleeding gums [5].
Monitor medication safety if a patient is taking prescription blood thinners like warfarin [1].
What Doctors Are Trying to Learn
Physicians utilize your INR to measure the actual manufacturing power of your liver and evaluate your systemic protection against bleeding [2]. When a liver becomes heavily scarred from cirrhosis, its factory slows down, and it produces fewer clotting factors [3]. Fewer clotting factors mean it takes a longer time for your blood to successfully plug a blood vessel leak, causing the INR number to climb upward [4].
Hepatologists are also trying to learn how your INR is communicating with your platelet count [3]. While your platelets are physical cellular fragments that act as the structural “bricks” to plug a bleed, the clotting factors measured by your INR act as the chemical “cement” that binds those bricks together [2]. By looking at both tests, doctors gain a complete understanding of your true coagulation profile [4].
How to Prepare
An INR blood draw is highly routine and requires very little specialized physical preparation:
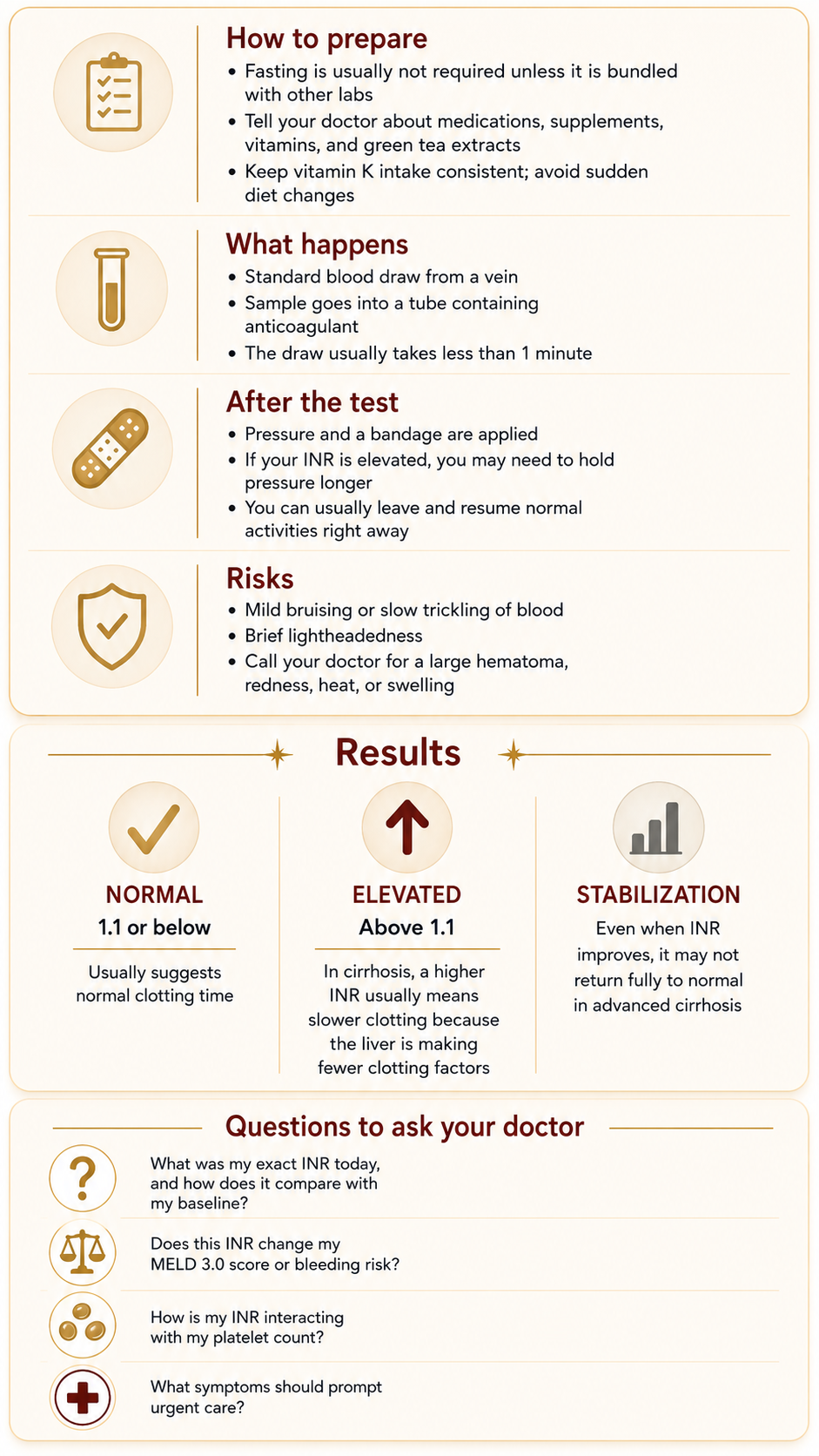
Fasting Requirements: Fasting is typically not required if you are only running a PT/INR test, but an 8-to-12-hour fast is standard if it is bundled into a broader metabolic panel [5].
Medication Disclosures: It is vital to tell your doctor about all daily medications, supplements, and vitamins you take. Compounds high in Vitamin K, green tea extracts, or everyday pain relievers can directly skew clotting data [1].
Consistency in Diet: Avoid sudden, drastic changes in your intake of green, leafy vegetables directly before the test, as these are rich in Vitamin K and can temporarily alter your blood’s clotting capabilities [2].
What Happens During It
The test is a standard needle stick, or venipuncture, performed by a healthcare professional [5]. An elastic band is wrapped around your upper arm to isolate a vein, the skin is sterilized with an antiseptic wipe, and a small needle is inserted [1]. The blood is drawn into a specific collection tube containing an anticoagulant to preserve the sample, and the draw finishes in under a minute [5].
What Happens After It
Once the needle is removed, a sterile gauze pad is applied to the puncture site [5]. Because an elevated INR directly means your blood takes longer to clot, you will likely need to hold firm pressure on the gauze significantly longer than a standard patient to ensure the bleeding has stopped completely before an adhesive bandage is applied [4]. Afterward, you can leave immediately and resume your normal daily activities [1].
Risks and What to Watch For
An INR blood test carries a very safe profile with minimal risks [1]. Temporary localized side effects can include:
Mild bruising or prolonged trickling of blood around the exact venipuncture site [5].
Brief lightheadedness during or immediately following the stick [2].
Signs to report: Call your doctor if you experience rare complications like a large, expanding lump under the skin, called a hematoma, or signs of infection like spreading redness, swelling, or heat at the needle site [5].
What Results May Mean
For a healthy individual who is not taking blood-thinning medications or living with liver disease, a standard normal INR value is typically 1.1 or below [1].
Normal Range: 1.1 or below
This suggests that the liver is synthesizing a healthy, adequate supply of clotting proteins and the body can form a stable fibrin clot within standard time limits [2].
Elevated Levels: Above 1.1 to 2.0+
In a cirrhosis patient, an elevated INR means the liver’s manufacturing capacity has slowed down due to parenchymal scar tissue [3]. When the number climbs to a 2.6 or 2.7, it signals a significant delay in clotting time and a high clinical urgency, directly raising your priority on the MELD 3.0 transplant score list [4].
The Stabilization Reality
Through healthy lifestyle adjustments, medications, and medical management, a severely elevated INR can improve and trend down to a lower, much safer range. However, because advanced structural changes remain in a cirrhotic liver, the INR may permanently live slightly out of bounds, meaning you must maintain continuous, careful lifestyle awareness regarding bleeding hazards [3].
Questions to Ask Your Doctor
To help you track your clinical trends and advocate for your health at your next medical visit, consider bringing these specific questions to your provider:
What was my exact INR value on today’s lab panel, and how does it compare to my baseline over the last six months?
Given my current INR number, are my daily bleeding risks stable, or should I be taking extra physical precautions to avoid minor injuries?
How is my current INR interacting with my platelet count to protect me against spontaneous bleeding or bruising?
How does today’s INR value affect my current MELD 3.0 score calculation or my overall disease staging?
What specific signs—like a certain duration of a nosebleed or specific dark stools—should prompt me to seek immediate emergency care based on my clotting time?
Sources
Source 1: Mayo Clinic: Prothrombin Time Test and INR Overview, Clinical Purpose, and Reference Intervals
Source 2: Cleveland Clinic: Understanding the International Normalized Ratio (INR), Clotting Factors, and Coagulation
Source 3: Journal of Hepatology: Consensus Guidelines on Liver Synthetic Function, Coagulation Profiles, and MELD Scoring Staging in Cirrhosis
Source 4: The American Journal of Gastroenterology: ACG Clinical Guideline: Comprehensive Evaluation of Abnormal Liver Chemistries, Coagulation Testing, and Bleeding Risk Factors
Source 5: National Institutes of Health (NIH) / MedlinePlus: Prothrombin Time (PT/INR) Blood Test Protocols, Sample Collection, and Patient Safety