
Sodium

@diagnosis_cirrhosis 🧪🩸ALT explained: the liver lab that says “this is me” 👀💥 why is my doctor checking ALT? 🤔 what does a high ALT mean? 📈 is ALT liver damage? 💥 why is ALT high with fatty liver? 🍩 can alcohol raise ALT? 🍷 can meds raise ALT? 💊 why isn’t ALT in MELD? 🧮 ALT lives inside liver cells 🧬 so when it goes up ⬆️ 👉 it usually means liver cells are being injured and leaking it out 🩸🧪 not maybe ❌ not somewhere else ❌ 👉 this one is me 🫀 — 💥 what it means ALT goes up when liver cells are actively getting hurt 🍩 fatty liver (MASLD / NAFLD / MASH / NASH) 🍷 alcohol-related liver disease 💊 medication or supplement-related injury 🦠 hepatitis B or C 🔥 autoimmune hepatitis 🧬 bile duct and metabolic conditions 👉 different causes… same signal: cell injury 💥 — 📈 why ALT can move a lot ALT is an injury marker 🚨 so it can: ⬆️ spike when something is actively irritating the liver ⬇️ come down when that stress improves 👉 it reflects what’s happening right now, not the full long-term picture 👀 — 🧮 why it’s not in MELD MELD is about: 👉 overall liver function + survival risk ALT is about: 👉 active injury so even very high ALT 📈 doesn’t always mean the liver is failing — 💚 why this matters if ALT is elevated… 👉 something is actively affecting your liver but the real question is always: 👉 what is causing the injury? — 🧬 causes of liver damage (big picture) autoimmune hepatitis 🔥 fatty liver disease (MASLD / NAFLD / MASH / NASH) 🍩 alcohol-related liver disease 🚫🍷 hepatitis B 🦠 hepatitis C 🦠 primary biliary cholangitis (PBC) 🧬 primary sclerosing cholangitis (PSC) 🧬 hemochromatosis ⚙️ Wilson’s disease 🪙 alpha-1 antitrypsin deficiency 🧩 drug-induced liver injury 💊 👉 many different causes… but ALT rises when liver cells are taking a hit 💥🫀 — 👩⚕️🩺 talk to your doctor if ALT is elevated or changing 📈📉 👉 don’t guess the cause 👉 don’t assume it’s one thing your doctor will look at: 🧪 other labs (AST, bilirubin, ALP, GGT) 📊 trends over time 🧬 your history + medications because ALT is a clue… not the full answer 🧩 — ✨ real talk ALT can look scary because it moves 📈📉 but it’s your liver saying: 👉 “I’m the one getting hurt right now.” 💥 and that’s always worth paying attention to 👀 💚 #bloodwork #phlebotomist #liverhealth #patienteducation #medicaltiktok ♬ original sound - diagnosis cirrhosis
Top 4 Sodium Need to Knows
Important Medical Disclaimer: I am Angie, a cirrhosis patient sharing my personal lifestyle, nutrition, and mindset journey. I am a data aggregator and community builder, not a licensed medical professional, doctor, or dietitian. Content on diagnosiscirrhosis.com is based solely on my personal experience living with advanced liver disease and is intended for informational and educational purposes only. It does not constitute medical advice or a substitute for professional medical care. Always follow the recommendations of your own healthcare team and consult your hepatologist or physician before changing your diet, medication, or lifestyle routine.
My Experience with It
By Angie from @Diagnosis_Cirrhosis on TikTok
Once I figured out my little trick — ALT means “Always Liver” — I became convinced this number was going to be my gateway lab.
The one.
The number that would pull back the curtain and tell me exactly what was happening inside my body.
And then, because cirrhosis loves nothing more than ruining a clean theory, ALT did not behave quite how I expected.
For me, ALT has not been wildly dramatic. It has not been this flaming emergency flare shooting across my lab portal every other week. A lot of the time, I found myself staring at it, waiting for some massive spike or obvious explanation that never really arrived.
And to be clear, I am not giving a medical appraisal here. I am telling you how confusing it felt as a patient.
Because when you first start learning labs, you want one number to be the Rosetta Stone. You want one enzyme to say:
Here.
This is what is happening.
This is why you feel this way.
This is whether you are getting better or worse.
But ALT does not always give you that kind of theatrical performance.
At least mine did not.
Personally, ALT and AST often move in the same general direction, but I did not have the huge dramatic enzyme spikes I had read about online. And that was its own kind of confusing, especially while I was stabilizing and trying to understand what mattered.
So yes, ALT is a major clue.
But it has not been the singular secret decoder ring I expected it to be.
The other piece I have learned is that there is a balance between medical expertise and knowing your own body.
For example, a “spike” for me is to 80. Not the triple digit theatrics most expect. but for me, that’s “alarming”.
It’s important to have your own sense of a relative range. Whether your ALT tends to live around 15, 35, 65, or somewhere else entirely, it helps to know what your “normal for me” looks like.
Not because you are replacing your doctor. Absolutely not.
But because trends need context.
Your doctor knows medicine. You live in your body. Both pieces matter.
At the end of the day, ALT carries a lot of emotional weight for a tiny little enzyme.
It’s easy to look at ALT like it is supposed to walk into the room carrying the whole answer. And sometimes it brings something useful.
But sometimes it is just one flickering light on a very large dashboard.
So yes, respect it. Watch the trend. Ask your doctor what movement actually matters for your body. But do not make one tiny enzyme become the courtroom, the witness, the verdict, and the sentence.
Why Isn't in the MELD ?
@diagnosis_cirrhosis 🧪📊 Why aren’t AST and ALT part of the MELD score? One of the most frustrating things about liver disease is looking at your labs and feeling like the numbers are arguing with each other. Maybe your AST and ALT are sky-high, but your MELD barely moves. Maybe your enzymes improved, but you still feel awful. Maybe you’re wondering why your doctor doesn’t care about ALT and AST for transplant the way you do, or why a MELD score can affect transplant priority while liver enzymes are not even in the calculation. If you’ve ever felt like the numbers are speaking two different languages, you’re not alone. Because they are. — 🚗 Think of AST and ALT as a hail storm. Think of MELD as whether the car still runs. AST and ALT tell you: 🌩️ How hard is the car getting hit right now? MELD tells you: 🚗 Does the engine still work? Those are different questions. — When liver cells are injured, they leak AST and ALT into the bloodstream. That can happen with viral hepatitis, autoimmune hepatitis, medication injury, alcohol-related hepatitis, or fatty liver inflammation. The hail storm can be enormous. A massive hail storm can crack the windshield, dent every panel, destroy the paint, and make the car look terrible… while the engine still starts perfectly. That’s why people ask: 👉 Why are my ALT and AST high but my MELD score is low? 👉 Why doesn’t a high ALT and AST make my MELD score high? Because injury and function are not the same thing. The liver may be taking a beating, but it may still be functioning. — This is also why transplant teams don’t prioritize based on AST and ALT. It feels strange because higher enzymes seem like they should mean a sicker liver. But transplant is not asking: ❌ How much damage is happening today? It is asking: ⚠️ How likely is this person to die if nothing changes? That is the purpose of MELD. So when people ask: 👉 Why doesn’t my doctor care about ALT and AST for transplant? 👉 Why aren’t enzymes important for mortality risk? The answer is that AST and ALT are good at detecting injury, but much weaker at predicting survival. Someone can have AST and ALT in the thousands from acetaminophen overdose, hepatitis A, acute viral hepatitis, or drug-induced liver injury and still recover completely if the liver keeps functioning. — So why aren’t AST and ALT included in the MELD score? Because MELD was built around mortality risk. It uses: 🟡 bilirubin — can the liver clear waste? 🩸 INR — can the liver make clotting proteins? 🫘 creatinine — are the kidneys still working? 🧂 sodium — how disrupted has circulation become? Those predict survival better than enzymes. — Now flip it around. If my liver is failing, why are my enzymes normal? Because AST and ALT measure active destruction, not remaining capacity. In advanced cirrhosis, there may not be many healthy liver cells left to leak enzymes. So AST and ALT can look normal while bilirubin rises, INR rises, kidney function worsens, sodium falls, and the “engine” is failing. That is what MELD is watching. — And this is why MELD can feel disconnected from real life. If you have a MELD of 9 or 10 and still feel terrible, you are not crazy. MELD does not directly measure ascites, edema, fatigue, weakness, hepatic encephalopathy, or how much cirrhosis has taken over your daily life. So when people ask: 👉 Why doesn’t MELD capture how I actually feel? 👉 Why do I feel terrible if my MELD is low? The answer is that MELD measures mortality risk. Not quality of life. — AST & ALT: 🌩️ How bad is the hail storm? MELD: 🚗 Does the car still run? One measures active injury. One measures remaining function. One measures damage. The other mortality risk. And that’s why they don’t always agree. 👩⚕️👨⚕️🩺 Always talk to your doctor or hepatologist about AST, ALT, bilirubin, INR, creatinine, sodium, MELD score, Child-Pugh score, transplant eligibility, and what those numbers mean in your specific situation. #liverhealth #livertransplant #hepatitis #fattyliver #bloodwork ♬ The Mountain - FASSounds
It feels entirely backwards when you first discover that the MELD score—the definitive medical algorithm used to rank patients for organ allocation—completely locks ALT out of the equation [2].
The biological reality behind this decision rests on a crucial distinction: ALT is a localized leakage enzyme that reveals cellular inflammation, not an index of macro-level organ failure [1,5]. A surge in ALT simply means that hepatocyte membranes are currently compromised or rupturing, but it fails to communicate to the transplant calculator how much working liver mass is actually functioning to sustain life over the critical 90-day window [Source 4]. The MELD metric is unyielding in its focus, engineered solely to calculate imminent mortality risk.
Furthermore, relying on ALT would corrupt the data pool with highly volatile, non-hepatic noise. Because ALT is sensitive to a wide range of external, everyday variables—ranging from sudden shifts in body mass index (BMI) to minor metabolic changes or the introduction of a new over-the-counter drug—weaving it into the math would create chaotic fluctuations, rendering the patient priority list erratic and medically unsafe [2, 4].
Incorporating ALT would also cause catastrophic errors in patient prioritization due to the phenomenon of liver burnout [Source 3]. In cases of end-stage, terminal cirrhosis, the liver becomes so profoundly replaced by fibrotic scar tissue that the body's baseline reservoir of healthy hepatocytes is physically depleted [3, 4]. Because there is a drastic shortage of viable cells left to burst open, a patient on the brink of complete liver collapse can present with an ALT reading that appears flawlessly normal, masking their true clinical urgency [1, 5].
If triage networks based their decisions on ALT, individuals experiencing transient, self-limiting liver flares would mistakenly jump to the front of the line, while terminal patients with burnt-out, non-functioning livers would be ignored. To avoid this fatal flaw, the MELD formula bypasses these deceptive cell-injury markers altogether, choosing instead to evaluate true operational capacity through stable, life-sustaining indicators like bilirubin filtration, creatinine clearance, and INR clotting speed [3].
Key Takeaways:
What the Procedure Is
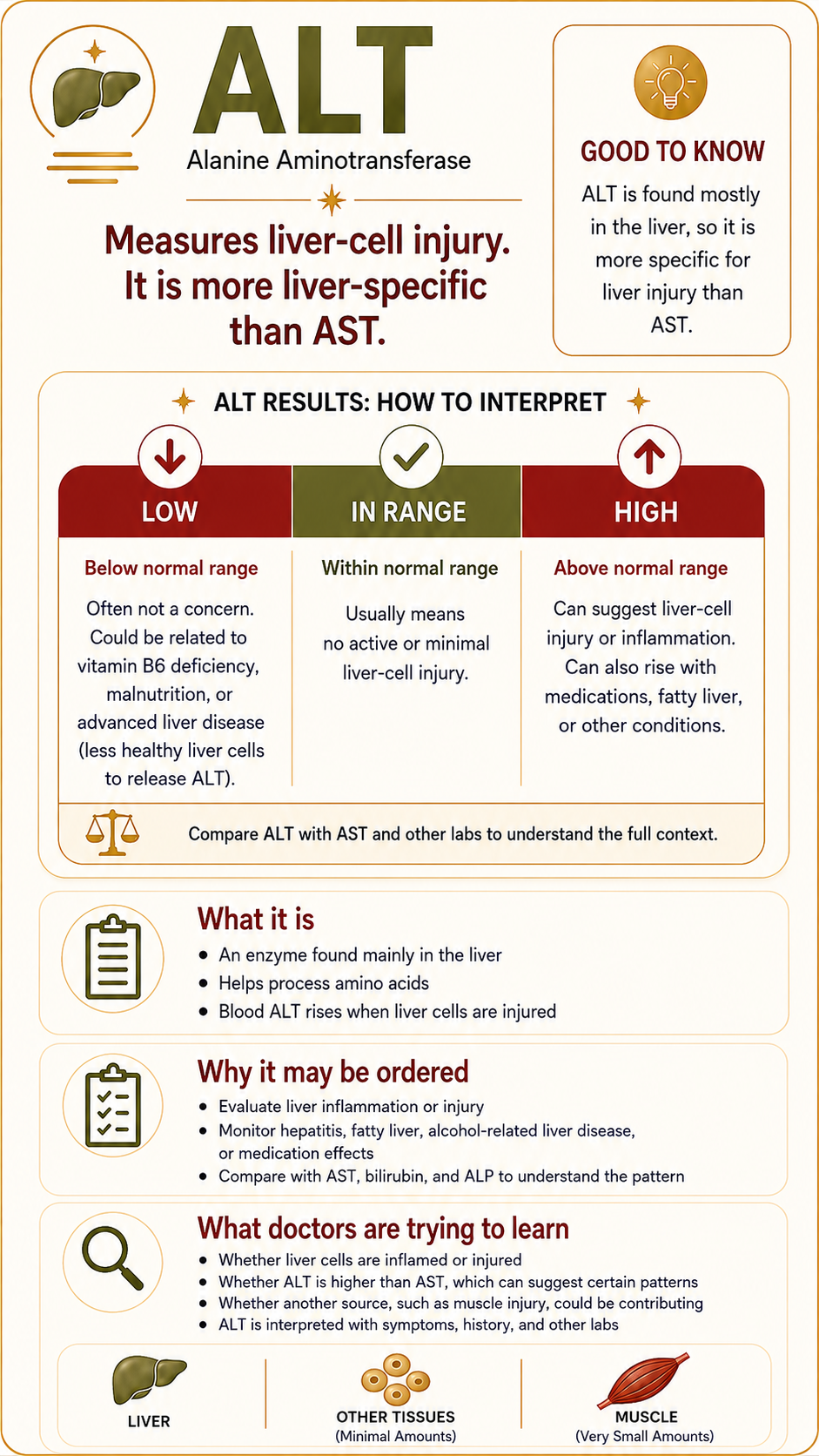
The Alanine Aminotransferase (ALT) test is a standard blood test used to measure the concentration of the ALT enzyme in your plasma [1]. Unlike AST, which is split among several organs, ALT is heavily concentrated inside the cells of the liver [2]. Because of this high specificity, it is considered one of the most reliable direct indicators of hepatic cellular integrity available in routine medicine [5].
Why This Procedure May Be Recommended
Your medical provider will utilize an ALT test to evaluate the physical state of your liver tissue. Clinical protocols recommend this test to [4]:
Investigate signs of hepatic illness, such as sudden jaundice, unexplained nausea, localized right-sided abdominal pain, or heavy fatigue [2].
Track chronic conditions, including metabolic dysfunction-associated steatotic liver disease (MASLD/NASH), chronic hepatitis B or C, or advanced cirrhosis [3].
Monitor drug safety to ensure your liver isn't being silently damaged by toxic reactions to prescriptions or heavy over-the-counter medication use [5].
What Doctors Are Trying to Learn
Physicians use the AST test to quantify the current scale of active cellular damage occurring in the body [2]. However, because AST is found in multiple organ systems, hepatologists rarely look at this value in a vacuum; they evaluate it alongside ALT (Alanine Aminotransferase), which is concentrated almost exclusively in the liver [1, 4].
By calculating the AST/ALT ratio, clinicians can better determine the specific root cause of the cellular stress [3]. According to clinical guidelines in the American Journal of Gastroenterology, a ratio where AST is significantly higher than ALT is a classic signature that points toward alcoholic liver disease or advancing fibrosis/cirrhosis, whereas a lower ratio where ALT dominates more frequently points to early-stage viral hepatitis or fatty liver disease [4].
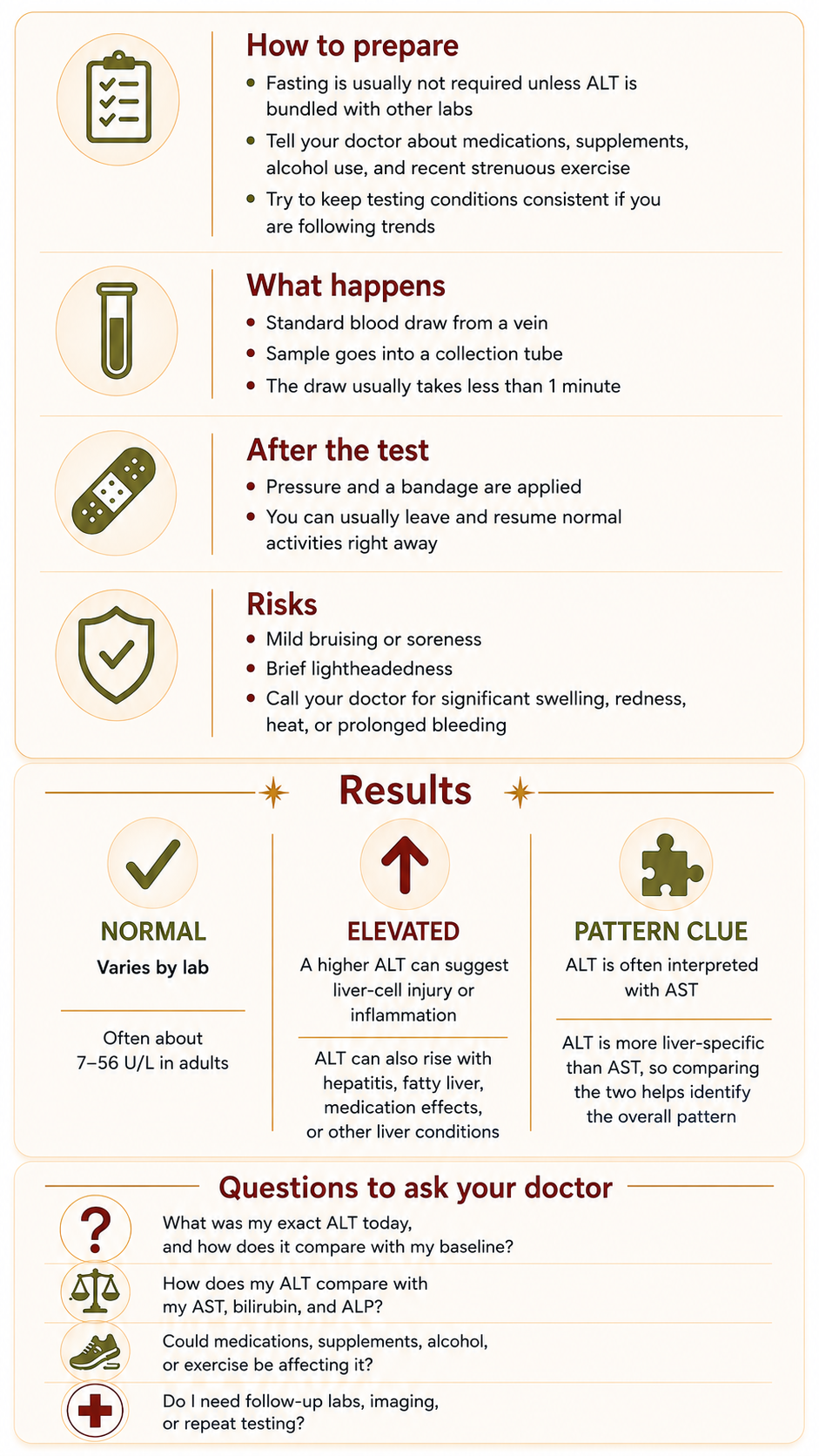
How to Prepare
An ALT blood draw is highly routine, but you should manage a few key details to keep your results accurate:
Fasting: You generally do not need to fast for an isolated ALT test, but an 8-to-12-hour fast is standard if it is part of a broader metabolic panel [5].
Supplement Disclosures: Always tell your doctor about every vitamin, herbal supplement, or over-the-counter medication you use, as many common compounds alter enzyme activity [2].
Exercise Rules: Avoid sudden, extreme physical overexertion right before your draw, as it can occasionally cause minor cross-reactive noise in your metabolic panels [1].
What Happens During It
The procedure is a standard needle stick (venipuncture) [5]. A healthcare professional cleans the skin at the crook of your elbow, applies a tight elastic band to locate a vein, and draws a small amount of blood into a sterile tube [5]. The process is over in less than a minute [5]. [1]
What Happens After It
A bandage is applied to the puncture site, and you are immediately free to leave [5]. There are no restrictions afterward; you can drive yourself home, eat right away, and continue your day normally [5].
Risks and What to Watch For
The physical risks of an ALT blood test are minimal and highly temporary [5]. They include:
Slight bruising or mild tenderness where the needle entered the vein [5].
Momentary lightheadedness during the draw [5].
When to call a doctor: While extremely rare, if you notice spreading redness, warmth, or swelling around the puncture site, you should contact your clinic to rule out an infection [5].
What Results May Mean
While exact reference ranges depend slightly on the specific laboratory analyzing the blood, normal ALT levels generally fall between 7 and 56 units per liter (U/L) [2].
Normal Levels: Indicate that there is no widespread, acute liver cell destruction or major active inflammation occurring right now [1].
Mild to Moderate Elevations: Frequently signal ongoing, manageable liver stress from conditions like a fatty liver, localized inflammation, or a mild reaction to a medication [2].
Severe Elevations (10x normal or more): Usually point to a sudden, acute liver emergency, such as an active viral hepatitis infection or acute liver poisoning (like an acetaminophen overdose) [1].
The Cirrhosis Flatline: Just like my personal experience, in advanced cirrhosis, your ALT numbers might not show huge, dramatic spikes [3]. Consensus guidelines point out that because chronic cirrhosis replaces healthy liver cells with permanent scar tissue, there are simply fewer active liver cells left to leak enzymes [3]. This is why a flat or near-normal number can sometimes mask advanced structural changes in the liver [4].
Questions to Ask Your Doctor
To help you understand your baseline and navigate your next appointment, consider asking your doctor these questions:
What is my current ALT number, and how does it compare to my personal baseline range?
Looking at my AST and ALT numbers together, what does our current ratio tell us about my cirrhosis progression?
Could any of my everyday prescriptions or over-the-counter supplements be keeping my liver enzymes elevated?
Since my ALT numbers aren't showing major spikes, what other tests (like a MELD score, platelets, or an ultrasound) are we using to verify my liver's actual stability?
What specific trends in these numbers should cause me to call your office between my regular yearly appointments?
Sources
[1] Mayo Clinic:Alanine Aminotransferase (ALT) Test Overview & Liver Health Screening
[2] Cleveland Clinic:Understanding ALT Levels, Liver Function, and Normal Reference Intervals
[3] Journal of Hepatology: EASL Clinical Practice Guidelines: Interpretation and Assessment of Laboratory Panels in Chronic Liver Diseases
[4] The American Journal of Gastroenterology: ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries and Enzyme Fluctuations
[5] National Institutes of Health (NIH) / MedlinePlus: ALT Blood Test Procedure, Clinical Interpretations, and Patient Risks
My Experience with It
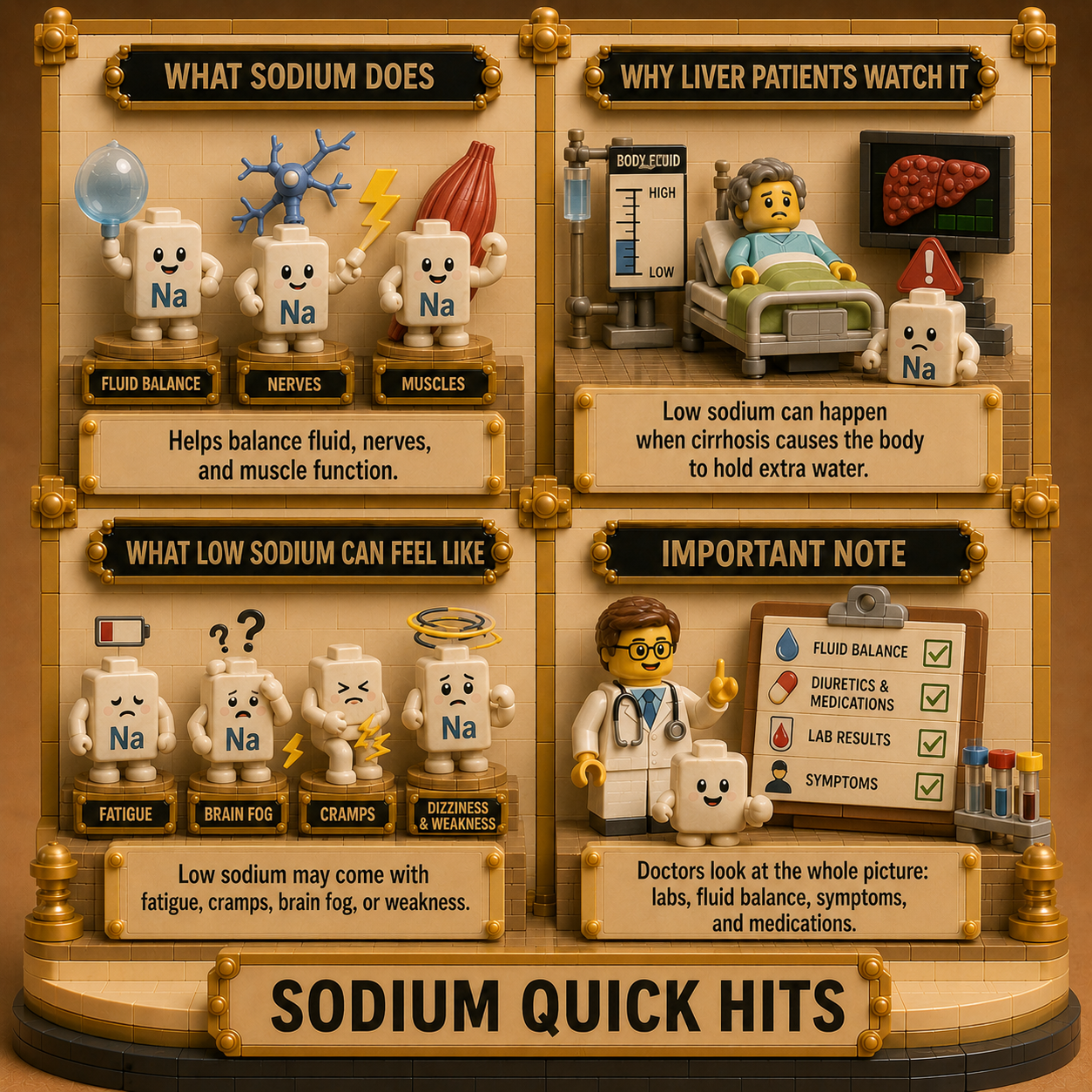
Sodium is like the artsy kid that nobody understands—you know, like in The Breakfast Club. It is the one that people look at and go, “Oh, duh, obviously I can name that. That is correlated to how much salt I’m having. Oh, it’s low because I’m on a low-sodium diet. Sodium? Oh, that’s easy, that’s easy, that’s easy.”
The thing about it is, it’s almost so obvious on the surface that the true dimension of it makes it even harder to understand. When you are on a low-sodium diet, when you are obsessed with sodium, when you are reading nutrition labels against your will—I mean, I’m not gonna act like it’s enjoyable, right?—and there is a headline of a nutrition label perpetually running in your head, you see “Sodium” show up on a CMP and you think, “Oh, this is easy, move on.”
But no. The reality is that serum sodium and dietary sodium are not the exact same thing. When you think about fluid balance and cirrhosis, all of the dynamics change. Understanding the element of dilution and how that factors into your sodium levels is everything. To get your serum sodium higher does not just mean consuming 4,000 or 5,000 milligrams of salt—which is completely off the table for us anyway!
This is a very important lab number, and it’s one that I wish I would have had the “aha” moment on much sooner. I spent a lot of time seeing myself in the red, staring at low numbers, and wondering, “Well, am I helpless? What can I even do about it? I’m being told that I can’t have sodium, yet my blood says it’s too low.” It felt like I was being punished or told I was doing a bad job, and that really was hard for me. I hope this article helps clear up that exact confusion for you.
What the Procedure Is
The serum sodium test is a foundational laboratory procedure that measures the concentration of sodium ions circulating in the liquid portion of your blood [1]. Sodium is an essential electrolyte and mineral that acts as the body’s primary extracellular solute [2]. This means it is the main osmotic force responsible for controlling the balance of water outside of your cells [5].
Why This Procedure May Be Recommended
A healthcare provider will routinely monitor your sodium levels via a basic metabolic panel or comprehensive metabolic panel [1]. In the context of liver health, clinical guidelines recommend this test to:
Calculate objective transplant scores, as serum sodium is a core variable built into modern staging models like the MELD 3.0 score [3].
Assess and manage fluid overload issues, including the development or worsening of ascites and peripheral edema [4].
Identify hyponatremia, or low blood sodium, a highly common and serious electrolyte complication in advanced chronic liver diseases [3].
Monitor the safety of diuretic therapies, like water pills, frequently prescribed to manage fluid retention [5].
What Doctors Are Trying to Learn
Physicians look at your serum sodium to judge the delicate relationship between water and salt in your blood vessels [2]. While a patient might assume a low sodium result means they need to eat more table salt, hepatologists view a low sodium level primarily as a sign of dilution [3].
In advanced liver disease or cirrhosis, portal hypertension causes the kidneys to inappropriately hold onto excess water [4]. This extra water stretches out the blood volume and physically dilutes the sodium that is already there [3]. By tracking this value, doctors are trying to learn how severely your liver condition is affecting your body’s hormonal fluid balance, which helps them fine-tune your fluid restrictions or diuretic medications [4].
How to Prepare
A sodium blood draw requires minimal preparation, but managing consistency ensures your lab data is accurate:
Fasting Requirements: Fasting is usually unnecessary if the sodium test is isolated, but you may need to fast for 8 to 12 hours if it is bundled into a broader metabolic panel [5].
Medication Updates: Inform your doctor about all current prescriptions, especially water pills, or diuretics, and blood pressure medications, as these can directly alter fluid retention and sodium handling [1].
Hydration Consistency: Drink a normal, baseline amount of water leading up to the test. Avoid sudden “chugging” of water or extreme fluid restriction right before the draw, as this can temporarily skew your concentration percentages [2].
What Happens During It
The procedure is a standard needle stick performed by a medical professional [5]. A phlebotomist or nurse ties an elastic band around your arm to map out a clear vein, cleanses the skin with an antiseptic wipe, and inserts a small needle [1]. The blood is collected into a sterile vacuum tube, and the active draw usually concludes in less than 60 seconds [5].
What Happens After It
Following the draw, pressure is applied to the puncture site with a sterile gauze pad to promote quick clotting, and an adhesive bandage is applied [5]. You are free to immediately leave the clinic, drive yourself home, eat, and continue with your day [1].
Risks and What to Watch For
A serum sodium blood draw carries an exceptionally safe profile with minimal clinical risks [1]. Temporary side effects are minor and may include:
Minor bruising or slight soreness around the exact vein where the needle entered [5].
A brief dizzy spell or mild vasovagal reaction during the draw [2].
Signs to report: Call your doctor if you experience rare complications like spreading redness, worsening throbbing pain, heat, or unusual swelling at the puncture site [5].
What Results May Mean
While reference intervals can fluctuate slightly depending on the individual laboratory analyzing your blood chemistry, standard normal ranges for serum sodium generally span 135 to 145 milliequivalents per liter, or mEq/L [1].
Normal Range: 135 to 145 mEq/L
This suggests that your body’s fluid-regulating systems are working in sync, maintaining a healthy equilibrium of water and salt in your bloodstream [2].
Elevated Levels / Hypernatremia: Above 145 mEq/L
This is less common in stable liver disease and typically points to severe systemic dehydration, a lack of fluid intake, or specific medication side effects [5].
Low Levels / Hyponatremia: Below 135 mEq/L
This is a major clinical signal in cirrhosis [3]. According to consensus guidelines published in the Journal of Hepatology, hyponatremia is rarely caused by a true shortage of salt in the body. Rather, it means the liver’s portal pressure is triggering the body to retain too much water, diluting your serum sodium [3].
While sodium is critical to compute priority in MELD 3.0, doctors do not treat it as just a calculator variable. Low numbers directly signal advanced fluid retention problems and tell doctors your body needs immediate clinical adjustments to stay safe [4].
Questions to Ask Your Doctor
To help bridge the gap between dietary tracking and your blood panel numbers, consider bringing these questions to your next appointment:
What was my exact serum sodium number today, and has it trended downward since our last panel?
Given that my sodium is out of range, is this a reflection of fluid dilution, or do we need to adjust my daily fluid restriction?
How is my current sodium level impacting my MELD 3.0 score calculation and my transplant status?
Are my current doses of water pills, or diuretics, contributing to this sodium level, or are they keeping it stable?
What specific signs of fluid retention, like weight gain or swelling, or neurological changes should I watch out for based on this result?
Sources
Source 1: Mayo Clinic: Sodium Blood Test Overview, Clinical Purpose, and Metabolic Panel Integration
Source 2: Cleveland Clinic: Understanding Blood Sodium Levels, Hyponatremia, and Electrolyte Balance
Source 3: Journal of Hepatology: Official Journal of the EASL - Clinical Practice Guidelines on the Management of Ascites, Spontaneous Bacterial Peritonitis, and Hyponatremia in Cirrhosis
Source 4: The American Journal of Gastroenterology: ACG Clinical Guideline: Comprehensive Diagnostics and Management of Liver Chemistries and Associated Fluid Complications
Source 5: National Institutes of Health (NIH) / MedlinePlus: Sodium Test Protocols, Sample Collection, Reference Ranges, and Patient Risks