
Albumin
Important Medical Disclaimer: I am Angie, a cirrhosis patient sharing my personal lifestyle, nutrition, and mindset journey. I am a data aggregator and community builder, not a licensed medical professional, doctor, or dietitian. Content on diagnosiscirrhosis.com is based solely on my personal experience living with advanced liver disease and is intended for informational and educational purposes only. It does not constitute medical advice or a substitute for professional medical care. Always follow the recommendations of your own healthcare team and consult your hepatologist or physician before changing your diet, medication, or lifestyle routine.
@diagnosis_cirrhosis 🧪📉 Albumin is not just “another lab” on your chart 👀📋 It is one of the main proteins made by the liver 🏭🧬 So when albumin starts dropping ⬇️ it can be a sign your liver is not working as well as it should ⚠️ Yes, albumin helps keep fluid where it belongs 💧➡️🩸 And when it gets low, fluid can start leaking into places it should not 😵💫 That can mean: ⚠️ swelling in the legs or feet 🦵 ⚠️ bloating 🤰 ⚠️ ascites 💧 ⚠️ feeling more run down or fragile 😞 But albumin is about more than fluid 👇 It also helps show how much liver function and support your body still has 🧠🫀🩸 That is part of why labs matter so much in advanced liver disease, cirrhosis, and liver failure 📊🩺 And it is also why newer scoring models like MELD 3.0 pay attention to albumin too 📉🧮 Your labs are not just numbers. They are clues 🕵️♀️✨ They help show what your liver is still able to do… and where it may be struggling 💛 Common causes of cirrhosis and chronic liver disease can include: alcohol-related liver disease 🚫🍷 fatty liver disease / NAFLD / MASLD 🍩🧈 NASH / MASH 🔥 hepatitis B 🦠 hepatitis C 🦠 autoimmune hepatitis 🛡️ primary biliary cholangitis 🧬 primary sclerosing cholangitis 🧬 hemochromatosis ⚙️ Wilson’s disease 🪙 alpha-1 antitrypsin deficiency 🧩 drug-induced liver injury 💊 and cryptogenic cirrhosis ❓ If you are living with cirrhosis, fibrosis, fatty liver, hepatitis, or unexplained symptoms, learning your labs matters 💡📚 Talk to your doctor or hepatologist if something feels off 👩⚕️👨⚕️🩺 #bloodwork #patienteducation #medschool #nursetok #liverhealth ♬ original sound - diagnosis cirrhosis
Top 4 Need to Knows:
My Experience with It
Albumin and I are relatively new friends.
It entered the vernacular before it was fluent in my vocabulary, if you will. I knew it was one of the numbers people cared about. I knew it was tied to how sick I was. I knew mine was bad.
But I did not yet understand that albumin was not just “protein” in the casual, chicken-breast-and-Greek-yogurt sense. I did not understand that it is one of the clearest windows into whether my liver was still able to manufacture what my body needed.
My first albumin was somewhere around 1.8 or 1.9, when the lower end of the standard normal range usually hangs around 3.4. So, in other words, not exactly a number that was out here inspiring confidence.
@diagnosis_cirrhosis 🧪🧬 What does albumin actually tell you? Why is it so important in cirrhosis? Albumin is one of the most important proteins your liver makes. It is not something you eat directly. It is not something your liver stores. It is a protein your liver manufactures using amino acids from the protein in your diet. So albumin reflects two things at once: 🏭 whether your liver can still manufacture proteins your body needs 🍽️ whether your body has the nutrition and building blocks to make them If you have ever wondered what albumin means in liver disease, why albumin is low with cirrhosis, can albumin improve during recompensation, what foods help albumin, or why albumin is included in MELD 3.0, this is the basic idea: Albumin is one of the clearest clues about liver function, nutrition, inflammation, fluid balance, and reserve. — 🏭 Think of your liver like a factory. Protein from food is broken down into amino acids. Those amino acids travel to your liver. Your liver assembles them into albumin and releases albumin into your bloodstream. If the factory has enough raw materials but damaged machinery, production can slow. If the machinery works but there are not enough raw materials, production can slow too. That is why albumin is influenced by both liver function and nutrition. — 💧 Why is albumin important? Most people hear “low protein.” But albumin does far more than that. Albumin helps keep fluid inside your blood vessels instead of leaking into surrounding tissues. When albumin is low, people may be more likely to develop or worsen: 💧 ascites 🦵 leg swelling / edema 🫁 fluid around the lungs in some cases Albumin also transports medications, hormones, fatty acids, minerals, and other important substances through the bloodstream. It is one of the hardest-working proteins your liver makes. — 📈 What does albumin tell doctors during recovery or recompensation? Recompensation means complications from decompensated cirrhosis have become controlled again. Not cured. Not scar-free. But more stable. If the underlying liver injury is controlled and the body stabilizes, albumin may slowly rise over time. Not because scar tissue disappeared. Because the remaining working liver tissue may be functioning better. An improving albumin trend may suggest: ✅ better liver synthetic function ✅ improved nutrition ✅ less inflammation ✅ better physiologic reserve ✅ more stable fluid balance Albumin usually does not change overnight. It has a half-life of about three weeks, so meaningful changes often take weeks to months. That is why the trend matters more than one isolated number. — 🥩 Can diet improve albumin? Nutrition matters. Your liver cannot manufacture albumin without amino acids. Adequate protein and calories give your body the building blocks it needs. But eating more protein does not automatically raise albumin. If liver synthetic function is reduced, inflammation is high, infection is present, kidney disease is causing protein loss, fluid overload is diluting labs, or total calorie intake is too low, albumin may stay low. So albumin is not just a nutrition score. It is a whole-body clue. — 🧮 Why is albumin in MELD 3.0? Older MELD and MELD-Na formulas did not include albumin. MELD 3.0 includes bilirubin, INR, creatinine, sodium, albumin, and sex. Albumin was added because it improves prediction of short-term mortality and transplant urgency. Low albumin can reflect reduced liver synthetic function, poor reserve, inflammation, nutrition issues, and fluid balance problems. 🧬 Chronic liver disease, liver damage, fibrosis, cirrhosis, and fatty liver disease may result from autoimmune hepatitis 🔥 fatty liver disease / MASLD / NAFLD / MASH / NASH 🍩 alcohol-related liver disease 🚫🍷 hepatitis B 🦠 hepatitis C 🦠 PBC 🧬 PSC 🧬 hemochromatosis ⚙️ Wilson’s disease 🪙 alpha-1 antitrypsin deficiency 🧩 drug-induced liver injury 💊 or many other liver diseases. #livehighlights #tiktoklive #liverdisease #liverhealth #bloodwork ♬ Coastline Drive - Nick Petrov
One of the stranger memories from those early days is how many doctors looked directly at me and said some version of:
“You will never be north of 3.0 again.”
Casually.
As if they were telling me the soup of the day.
And to be fair, they had reasons. At that point, my liver was not exactly submitting strong evidence in its own defense. But albumin is also one of those labs that people understandably misunderstand, because it sounds like eating more protein should fix it quickly.
And listen, protein intake matters. Nutrition matters. Preserving muscle matters. Please do not hear me saying otherwise.
But eating chicken breast does not immediately march into your bloodstream wearing a little albumin costume. That distinction matters because it keeps people from blaming themselves when albumin does not bounce back just because they are “doing everything right.” Yes, nutrition is part of the story. It is not the whole mechanism.
In my case, I have been incredibly fortunate. The number doctors warned me might never get above a 3 eventually climbed. Through stabilization, medication, time, and massive lifestyle changes, my albumin is recently north of 4.0.
For someone who started this journey with a MELD score around 30, that is not a small thing.
But it was not quick. It was not immediate. It was not a neat little reward sticker for eating enough protein.
It took a long, long time.
And even now, I try to remember that a 4 is not a guaranteed forever 4. Albumin can improve, but it can also move with illness, inflammation, fluid shifts, nutrition, kidney issues, and changes in liver status.
Why Albumin Matters in MELD 3.0
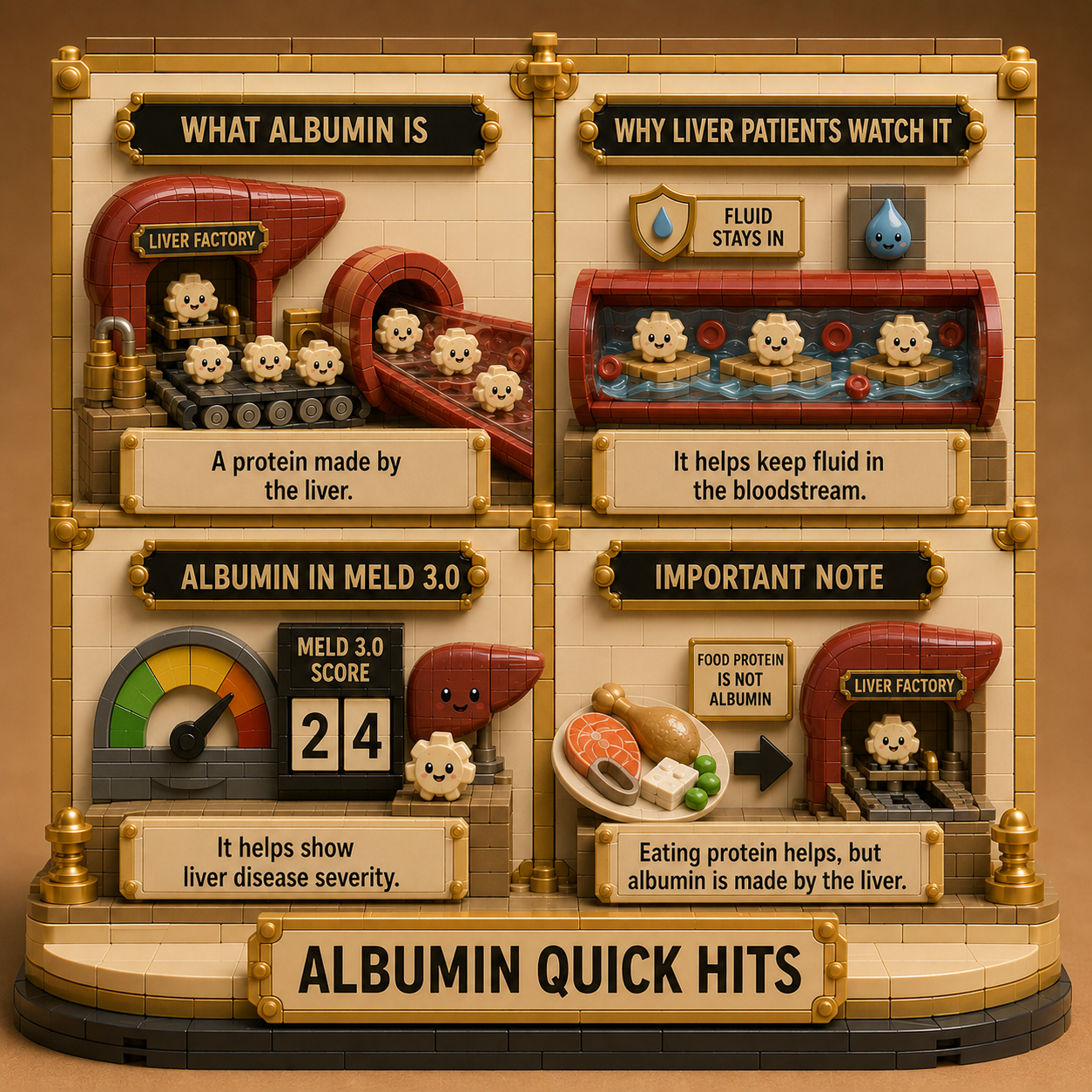
Albumin matters in MELD 3.0 because it helps show something bilirubin, INR, creatinine, and sodium do not fully capture on their own: whether the liver is still able to manufacture one of the major proteins the body depends on to keep fluid where it belongs [1].
That is the part I wish I had understood earlier. Albumin is not just a random protein number floating around on your labs [2]. It is one of the ways doctors can see whether your liver is still holding up its end of the bargain by evaluating its true synthetic, manufacturing health [4].
In MELD 3.0, albumin helps add more texture to the severity picture, especially because low albumin can reflect poor liver synthetic function, inflammation, malnutrition, fluid shifts, kidney issues, or the general instability that can come with advanced cirrhosis [3].
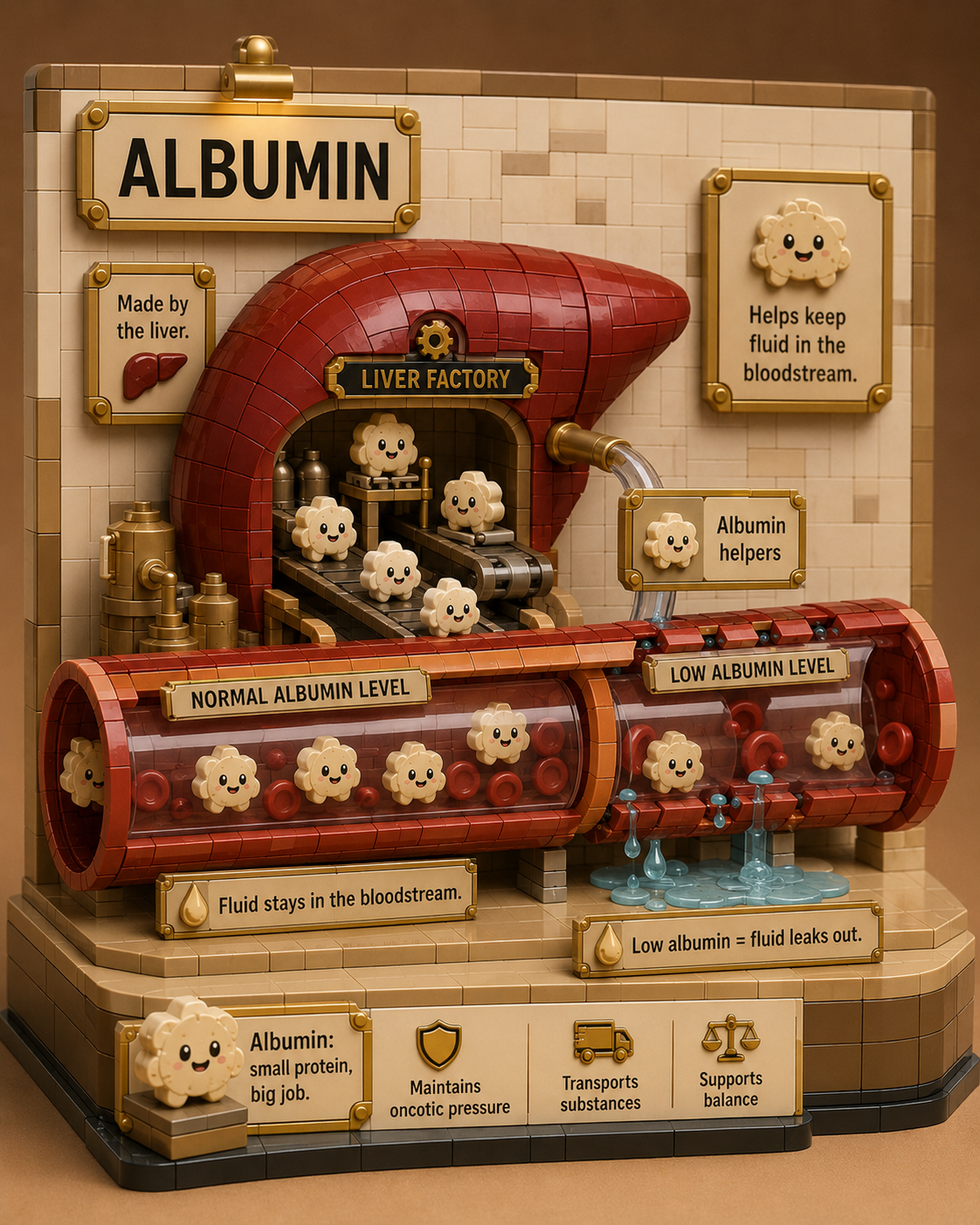
The way I think about it now is this: Albumin is the tiny fluid-holding sponge raft your liver is supposed to manufacture and send into the bloodstream [2].
When there are enough of those rafts, fluid is better held where it belongs inside your blood vessels due to proper oncotic pressure [1]. When the liver factory slows down and albumin drops, fluid has a much easier time leaking into places it does not belong, like the abdomen or legs, causing severe ascites or peripheral edema [3]. read about ascites specifically here
It is part nutrition, part liver manufacturing, part inflammation, part fluid balance, part disease severity, and part “how well is this whole system still holding together?” [4]. That is exactly why it belongs in the MELD 3.0 conversation to accurately calculate transplant priority and predict true short-term survival probability [3].
Key Takeaways:
What the Procedure Is
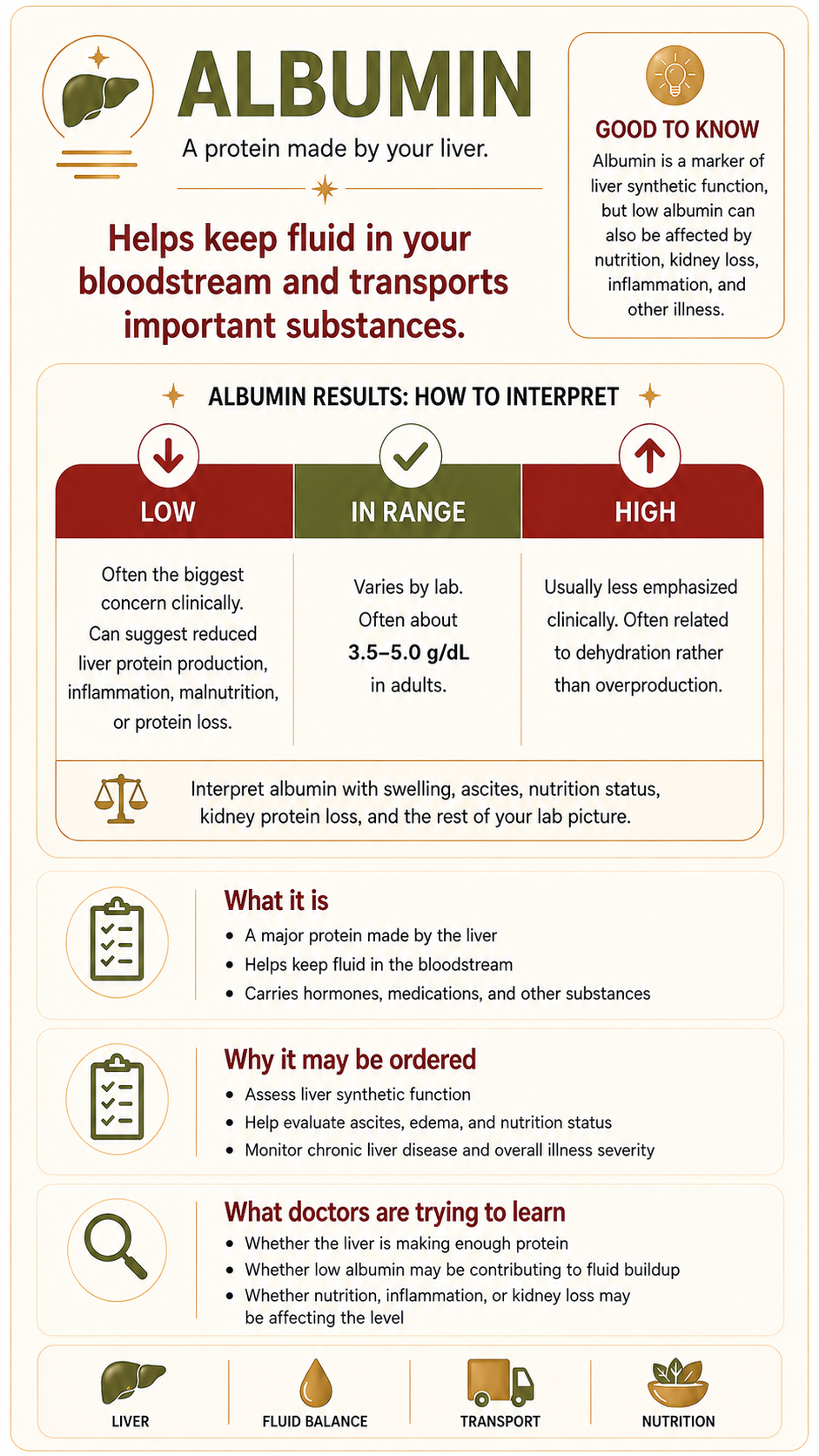
The albumin test is a routine laboratory blood test that measures the exact concentration of albumin in the liquid portion (serum) of your blood [1]. Albumin is a major plasma protein synthesized exclusively and entirely by the parenchymal cells of the liver [2]. It accounts for roughly 50% to 60% of all proteins actively circulating within human blood plasma [5].
Why This Procedure May Be Recommended
Because albumin can only be manufactured by functional liver tissue, a healthcare provider will order this test to evaluate the liver's direct manufacturing health [2]. Clinical protocols from organizations like the American College of Gastroenterology recommend this test to [4]:
Assess the liver's synthetic function when evaluating advanced, long-term chronic liver diseases like cirrhosis [3].
Calculate objective medical severity scores, such as the MELD-Na (Model for End-Stage Liver Disease) score or the Child-Pugh classification system, which heavily rely on albumin to determine transplant priority and disease staging [3, 4].
Investigate physical symptoms of fluid shifts, including severe ascites (fluid accumulation in the abdomen) or peripheral edema (swelling in the legs and ankles) [1].
Differentiate between nutritional deficiencies and actual organic organ failure [5].
What Doctors Are Trying to Learn
Physicians look at your albumin level to evaluate the true "working power" or synthetic capacity of your liver [4]. While basic liver enzymes like AST and ALT act as cellular flares that tell doctors cells are actively popping open, albumin tells doctors if the liver is successfully doing its daily manufacturing job [2, 4].
Furthermore, doctors use albumin to understand your blood's oncotic pressure—the magnetic force that keeps fluid safely inside your blood vessels instead of leaking out into your tissues [1]. When a hepatologist looks at your metabolic profile, they evaluate albumin as a directly measured metric alongside your "Total Protein" panel [2, 5]. By subtracting your direct albumin from your total protein, they get a calculated value for globulin (your immune system proteins), giving them a clear roadmap of both your liver's health and your body's inflammatory state [5].
How to Prepare
An albumin blood draw requires minimal physical preparation, but controlling baseline environmental variables keeps your numbers stable:
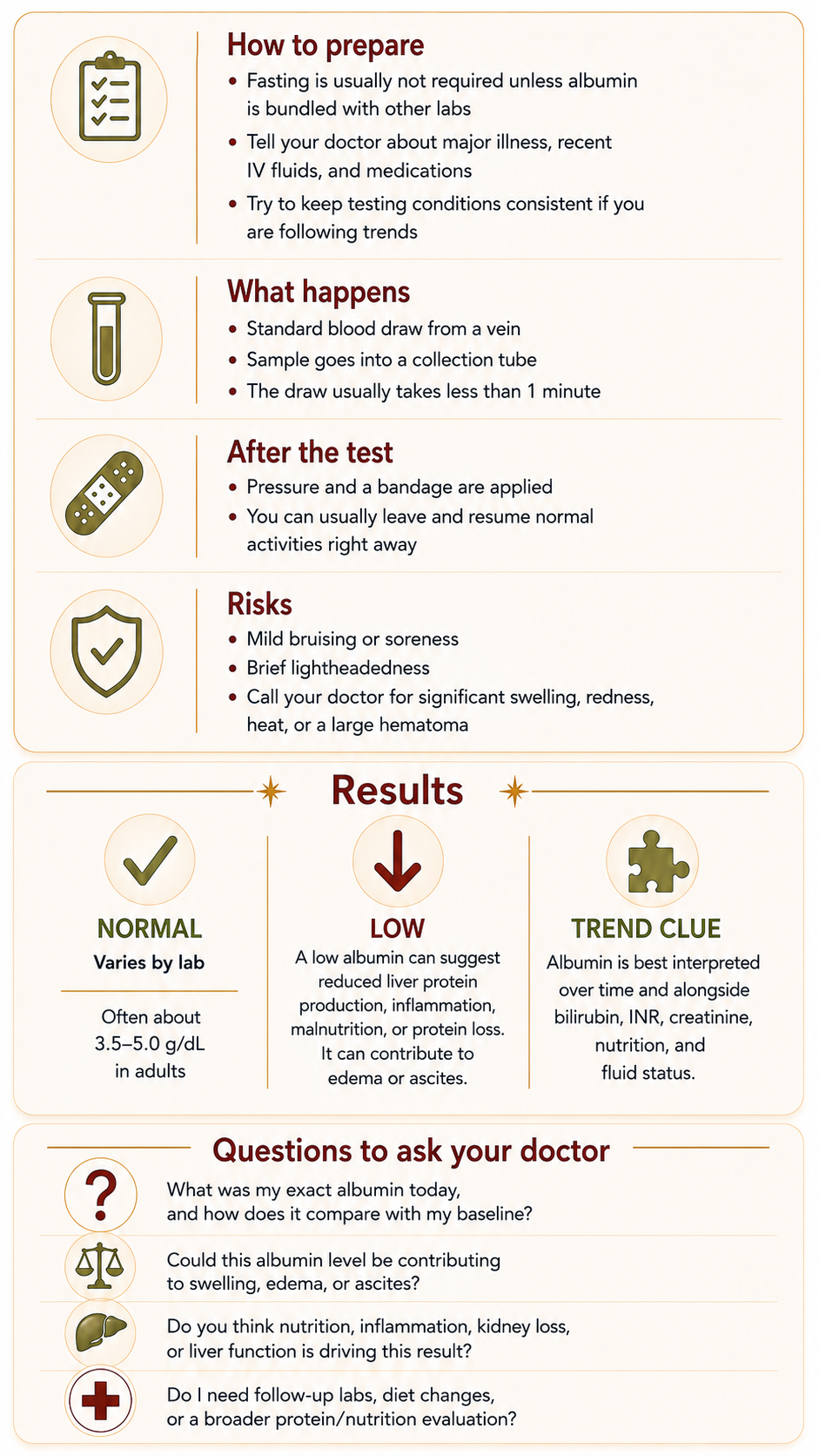
Fasting Requirements: Fasting is typically not required if albumin is drawn as an isolated test, but an 8-to-12-hour fast is standard if it is packaged into a larger comprehensive metabolic panel [1, 5].
Medication Disclosures: Tell your doctor about all prescriptions and over-the-counter drugs you take, as certain medications like anabolic steroids, growth hormones, or insulin can artificially distort your circulating protein levels [5].
Maintain Stable Hydration: Avoid severe dehydration or sudden fluid overhydration right before the test, as severe shifts in blood volume can artificially concentrate or dilute your protein percentages [1].
What Happens During It
The test is a standard needle stick (venipuncture) performed by a medical professional [5]. A phlebotomist or nurse will place an elastic band around your upper arm to locate a clean vein, sanitize the area with an antiseptic wipe, and insert a small needle [5]. The blood flows into a collection tube, and the needle is typically removed in under 60 seconds [5].
What Happens After It

Once the needle is withdrawn, a clean gauze pad is held against the site with light pressure to ensure clotting, and an adhesive bandage is applied [5]. You are free to leave the lab immediately, drive yourself home, eat, and continue your normal daily schedule [5].
Risks and What to Watch For
An albumin blood test carries an exceptionally low profile for clinical risk [1, 5]. Minor localized issues are temporary and may include [5]:
Slight bruising or light swelling at the exact point of the needle stick.
Brief dizziness or a mild vasovagal reaction during the active draw.
Complications to note: While vanishingly rare, if you experience spreading redness, intense heat, or throbbing pain around the vein puncture, contact your care team immediately to rule out localized infection [5].
What Results May Mean
While exact reference intervals vary slightly depending on the specific equipment your hospital or lab uses, standard normal ranges for serum albumin generally fall between 3.4 and 5.4 grams per deciliter (g/dL) [1, 2].
Normal Range (3.4 to 5.4 g/dL): Indicates that your liver possesses an adequate volume of healthy, unscarred parenchymal cells to synthesize vital proteins and maintain proper blood volume distribution [2, 3].
Elevated Levels (Above 5.4 g/dL): Are almost never caused by a hyper-functioning liver; instead, high albumin is a classic indicator of severe systemic dehydration [1, 2].
Low Levels / Hypoalbuminemia (Below 3.4 g/dL): Signal that the liver's manufacturing plant is falling behind due to structural damage [2, 4].
The Diet vs. Liver Reality: A common misconception among patients is that a low albumin level can be quickly fixed simply by eating more lean steaks or drinking protein shakes. In consensus guidelines published in the Journal of Hepatology, experts emphasize that in advanced cirrhosis, the bottleneck isn't a lack of dietary protein components coming in; it is that the liver's structural factory is heavily scarred and physically lacks the functional machinery to turn those amino acids into albumin [3]. When numbers drop to critical levels like 1.8 or 1.9, the blood loses its oncotic pressure, causing fluid to leak directly into the abdomen (ascites) or legs [1, 3].
Questions to Ask Your Doctor
To help track your personal baseline trends and advocate for your care at your next clinical visit, consider bringing these specific questions to your provider:
What was my exact albumin number today, and how does it compare to my baseline when I was first diagnosed?
Given that my albumin dropped/stalled, what does this tell us about the current structural factory capacity and synthetic function of my liver?
How is my direct albumin number interacting with my calculated globulin levels on my total protein panel?
Are my physical symptoms, like sudden ankle swelling or abdominal tightness, directly tied to my current albumin level dropping?
What lifestyle steps, medications, or monitoring can we implement to help support my liver tissue as we try to safely trend toward my target range?
Sources
[1] Mayo Clinic:Albumin Blood Test Overview, Clinical Application, and Fluid Regulation Roles
[2] Cleveland Clinic:Understanding Serum Albumin Levels, Total Protein Profiles, and Liver Health
[3] Journal of Hepatology: Official Journal of the EASL - Prognostic Significance of Albumin Synthesis and Portal Hypertension in Decompensated Cirrhosis
[4] The American Journal of Gastroenterology: ACG Clinical Guideline: Comprehensive Laboratory Assessment of Hepatic Function and Synthetic Staging
[5] National Institutes of Health (NIH) / MedlinePlus: Albumin Blood Test Protocol, Direct vs. Calculated Values, and Patient Safety