
MELD 3.0
By Angie from @diagnosis_cirrhosis on TikTok
Math of Mortality
The evolution from the original MELD score to MELD 3.0 represents a high-stakes, data-driven update to the math governing liver transplantation [1, 2]. For over a decade, the medical community relied on a standard calculation that, while revolutionary, contained critical structural blind spots. MELD 3.0 updates the logarithmic formula to fix systemic inequalities and capture a more accurate picture of multi-organ failure [1].
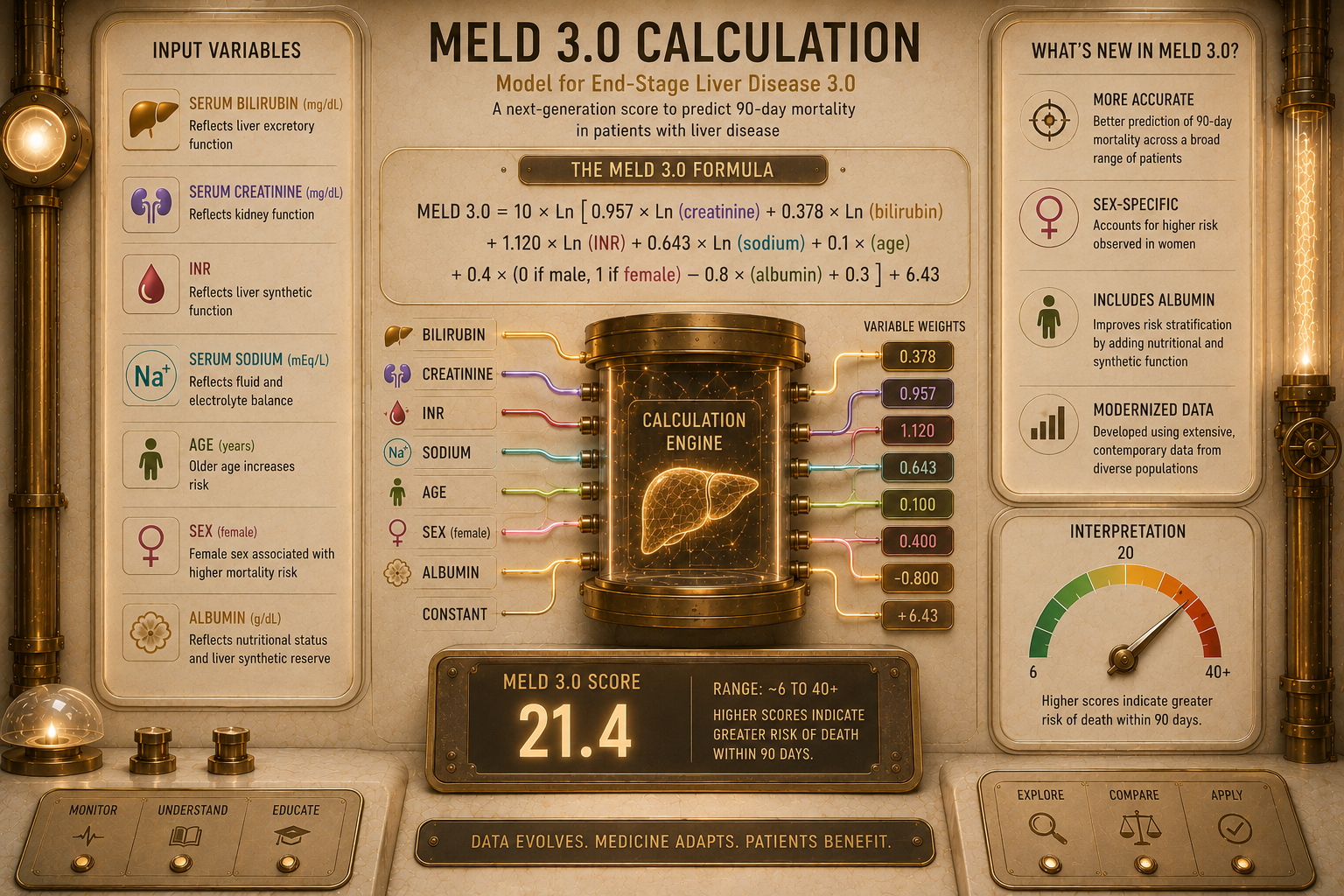
What’s New MELD 3.0 introduces three specific mathematical and variable updates to the calculation: [1]
MELD 3.0 introduces three specific mathematical and variable updates to the calculation [1].
The Gender Equity Coefficient: The updated formula applies a specific math correction to account for a patient’s biological sex. This variable automatically adds a baseline weighting coefficient (+1.33 points) for female candidates to prevent them from being structurally penalized by standard lab measurements.
The Serum Albumin Integration: Albumin—a primary protein manufactured by the liver to keepfluid from leaking out of blood vessels—is now explicitly woven into the equation as an independent, dynamic variable.
Lowered Creatinine Maximum Caps: The mathematical ceiling for serum creatinine (the kidneyfailure marker) has been lowered from 4.0 mg/dL down to 3.0 mg/dL within the internal calculation.
Dynamic Variable Interactions: The model introduces interactive terms that link variables together, specifically mapping the interplay between creatinine and albumin, as well as sodium and bilirubin. This accounts for how a drop in one marker severely amplifies the danger of another [1, 2].
Why It Matters These statistical adjustments address severe, real-world disparities in how organs were distributed:
These statistical adjustments address severe, real-world disparities in how organs were previously distributed:
Fixing the Muscle Mass Bias: The original MELD score relied heavily on creatinine to measure kidney health. Because creatinine is a byproduct of muscle breakdown, women—who generally possess less muscle mass than men—frequently showed lower creatinine levels on paper despite having identical, severe kidney impairment. This statistical bias meant women routinely received lower MELD scores, experienced higher death rates while waiting on the list, and had a lower chance of receiving a transplant [1, 2]. The female sex variable directly levels this playing field.
Tracking the True Fluid Collapse: Incorporating albumin provides an immediate, objective tracking metric for severe nutritional wasting (malnutrition) and fluid retention [1]. By pairing albumin with sodium, the score accurately identifies patients who are physically drowning in their own ascites fluid, even if their traditional blood-clotting markers appear temporarily stable.
Preventing the Kidney Math Bias: In the older MELD formula, once a patient's kidney failure caused their creatinine to hit 4.0 mg/dL, the calculation hit a hard limit. MELD 3.0 recognizes that severe kidney injury begins causing catastrophic systemic damage much earlier. Lowering the cap to 3.0 mg/dL ensures that early-stage kidney failure gives patients the appropriate priority boost on the waitlist before their entire body suffers irreversible shock [1].
The official legal and regulatory transition mandating all transplant clinics across the United States to collect and submit these expanded matrices was finalized by national policy updates [3].
Sources
The Validation Study: Kim, W. R., Mannalithara, A., Heimbach, J. K., Kamath, P. S., Asrani, S. S., Biggins, S. W., Wood, N. L., Gentry, S. E., & Kwong, A. J. (2021). MELD 3.0: The Model for End-Stage Liver Disease updated for the modern era. Gastroenterology, 161(6), 1887–1895. View in Gastroenterology Journal. [1, 2]
The Open Access Track: Kim, W. R., Mannalithara, A., Heimbach, J. K., Kamath, P. S., Asrani, S. S., Biggins, S. W., Wood, N. L., Gentry, S. E., & Kwong, A. J. (2021). MELD 3.0: The Model for End-stage Liver Disease Updated. National Institutes of Health PMC Archive, PMC8608337. Read Free via NIH PubMed Central. [1]
The Regulatory Policy: Organ Procurement and Transplantation Network. (2023). Improving liver allocation: MELD, PELD, Status 1A, Status 1B policy. Health Resources and Services Administration. Review the Official OPTN Implementation Guidance.