
Platelets

My Experience with It
Let’s be honest, guys: I think anyone who can easily read their Complete Blood Count (CBC) is on an advanced graduate level of cirrhosis knowledge—maybe multiple, multiple years in. I am at the year-and-a-half mark, and the CBC is still something I stumble through and struggle with. For some reason, the metabolic panels make so much more sense to me.
But I can tell you this: I am a falcon, laser-eyed, when it comes to a couple of specific parts on that CBC, and platelets are absolutely one of them. Platelets just make sense to me. When your platelets are low, it’s because they’re trapped in your spleen. I think of the spleen like a jailhouse, holding onto the platelets so they can’t rush out and plug up your bleeding or help with bruising. I know that’s not a perfect medical explanation, but the point is, I get why they are low. I can understand, track, and visualize the chemistry and the physiology of why it happens in my own body.
The thing about platelets, though, is that it is not a linear trajectory. Going from a count of 100 down to 90 is not the same thing as dropping from 60 down to 50. The lower your numbers get, the more you have to think about the density of those platelets and just how much of your body they are intended to cover.
For me, my platelets usually hang around 80 to 85. It’s not fabulous, but it’s not awful either. It is, however, something I have to be hyper-conscientious of every single day because the bleeding risk is real, the platelet trap is real, and this is just a fundamental part of living with cirrhosis.
I knew, intellectually, that bleeding could become part of the plot. I had varices. I had the warning labels. I understood that cirrhosis could make the body less talented at the whole “keep the blood inside” arrangement. But theory is very different from standing in your bathroom one evening, brushing your teeth, having just taken your medicine, wearing a sports bra and pajama shorts, and looking down to discover that your belly button is bleeding. Your belly button.
Not exactly the area I had ranked high on my internal list of possible crime scenes. There are certain Pollock-prone body parts one might expect to betray you, but the navel did not make my top three. So there I was, fully outside of my body, staring down like, excuse me? Since when did this particular region become a volcano?
Naturally, an ER visit ensued (caregivers guide to varices) ,because “spontaneous belly button bleeding” is apparently not something you just file under quirky and continue your evening. As it turned out, my platelets had dropped from around 100 to around 60 within a handful of days, which is exactly the kind of dramatic numerical betrayal that makes platelets feel less like a lab value and more like tiny chaotic employees abandoning their post without notice. It isn’t the most common thing, but they can move so it’s important to pay attention to any changes within your body and the signs/signals/salutations it’s providing. more on varices
Why They Aren't in the MELD Score
Even though platelets drop like a stone for the majority of us with advanced liver disease, they are completely missing from the standard MELD score calculation [1]. When you are sitting at home opening your lab portal, tracking a plummeting platelet count, and knowing the "spleen jailhouse" is actively trapping your cells, it can feel incredibly confusing and frustrating that this number doesn't raise your score or push you higher on the transplant list. It almost feels like the algorithm is ignoring a massive part of what makes you feel sick and fragile every single day.
The clinical reason for this omission comes down to what the MELD formula is designed to measure: absolute, short-term mortality risk across all different types of liver failures [3]. While a low platelet count is an excellent, highly reliable indicator that you have severe portal hypertension and an enlarged spleen, medical studies have shown that platelet numbers do not cleanly or predictably correlate with your direct three-month survival probability [4]. For example, two patients can have the exact same MELD score, but one might have a platelet count of 40,000 due to severe splenic sequestration, while another sits at 130,000—yet their immediate short-term survival risks remain statistically identical [3].
Furthermore, platelet counts fluctuate wildly based on specific variables that have nothing to do with how sick your actual liver factory is [2]. Platelet counts can drop because of bone marrow production issues, viral exposures, or a history of alcoholic liver injury, making it too inconsistent to be used as a standardized, universal metric for ranking everyone fairly on a national organ waitlist [5]. The MELD formula deliberately leaves them out to prevent these non-linear, external variables from skewing the fairness of the scoring system [3]. So, while platelets are a critical lifetime tracking number for your everyday bleeding and bruising safety, the MELD score sticks strictly to labs that directly map active organ failure, like your bilirubin and INR [2].
What the Procedure Is
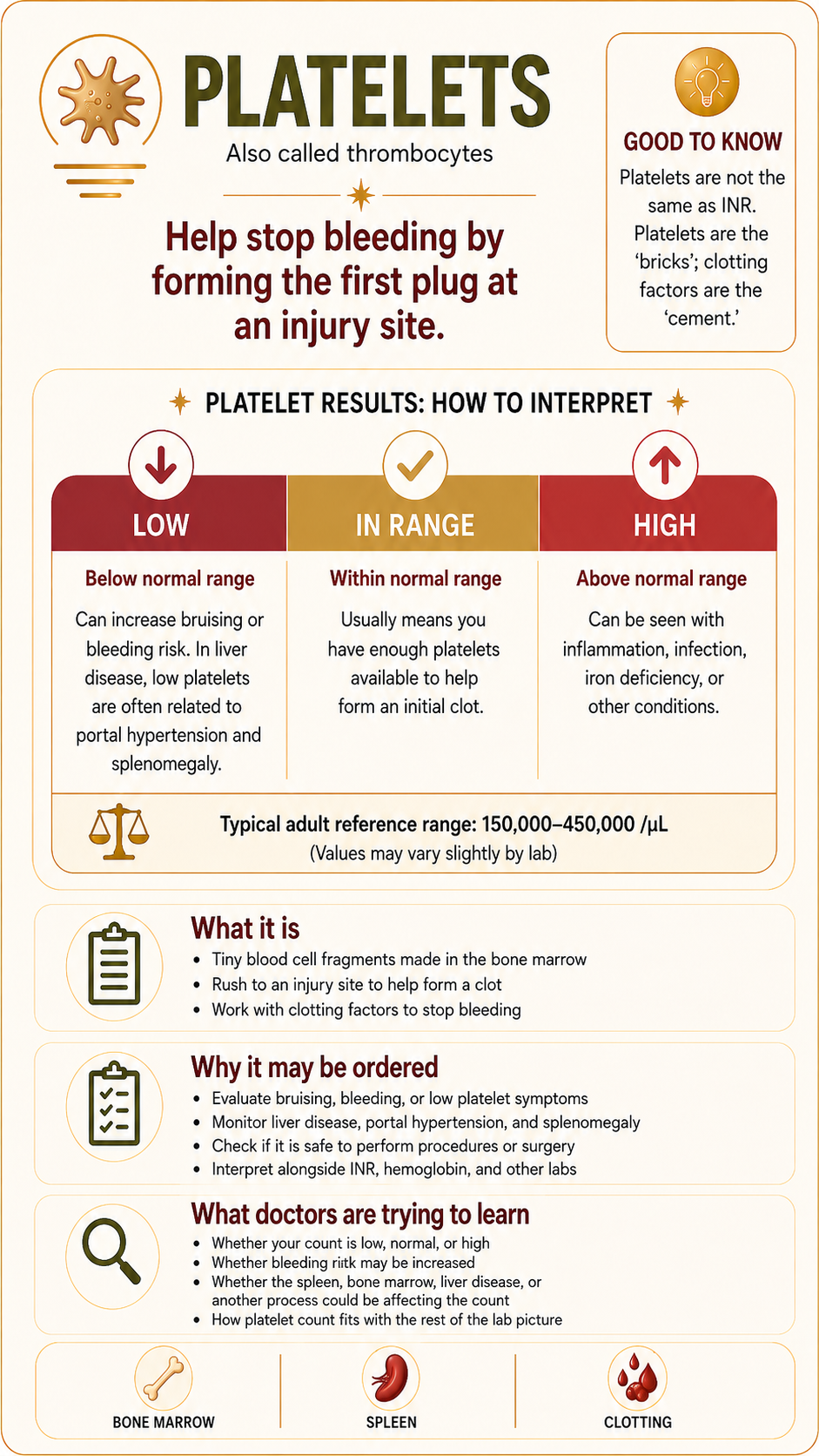
The platelet count test is a standard component of a Complete Blood Count, or CBC, which is a routine blood panel utilized to evaluate overall hematologic health [1]. Platelets, legally termed thrombocytes, are tiny, disc-shaped cellular fragments manufactured within your bone marrow that circulate dynamically through the bloodstream [5]. Their primary cellular responsibility is to aggregate and bind together at the site of a damaged blood vessel to form a physical haemostatic plug, halting active bleeding and initiating the cascade required for wound healing [2].
Why This Procedure May Be Recommended
Your medical provider will order a CBC containing a platelet count to evaluate your physiological clotting status. In individuals navigating chronic hepatic diseases, clinical guidelines recommend this test to:
Screen for occult portal hypertension, as a steadily dropping platelet count is frequently the very first measurable sign that pressure is building up in the liver’s vascular system [3].
Assess bleeding and bruising risks prior to undergoing any planned surgical treatments, dental work, or invasive screening procedures like an endoscopy [4].
Monitor the progression of advanced liver damage, as platelet counts help clinicians track structural severity and fibrosis over time [3].
Evaluate unexplained physical symptoms, such as spontaneous nosebleeds, bleeding gums, or petechiae—which are pinhead-sized red or purple dots on the skin caused by minor capillary bleeding [5].
What Doctors Are Trying to Learn
Physicians look at your platelet count to judge how well your body can defend itself against internal or external bleeding complications. In a completely healthy body, the spleen acts as a minor reservoir, temporarily holding onto about one-third of your circulating platelets for active use [2].
However, in advanced liver disease or cirrhosis, extensive scar tissue physically blocks the smooth transit of blood flowing through the liver. This major backup of blood creates intense backward pressure, known as portal hypertension, which forces the spleen to significantly expand in size—a clinical condition called splenomegaly [3]. The enlarged spleen turns into an overactive “jailhouse,” capturing and trapping up to 90% of the body’s entire platelet supply inside its tissue walls, keeping them completely out of the active bloodstream where they are needed to prevent bruising [4].
By tracking your platelets, doctors are trying to learn the exact severity of your portal hypertension and evaluate your current safety margin against bleeding [3].
How to Prepare
A standard platelet count via a CBC requires very little physical preparation, but keeping your variables controlled ensures your baseline data is highly accurate:
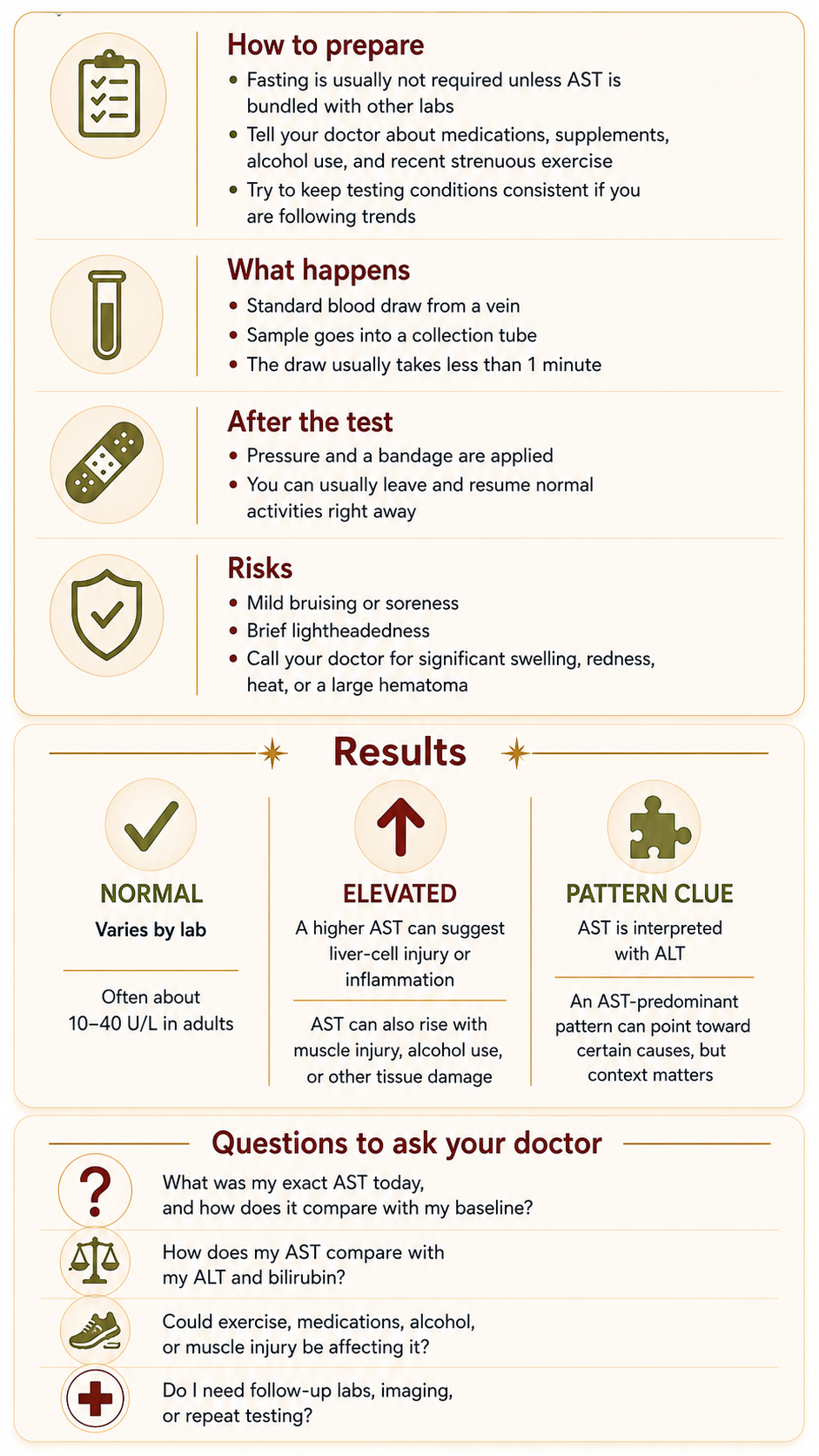
Fasting Requirements: Fasting is not required if you are only receiving an isolated CBC, though you will need to fast for 8 to 12 hours if it is bundled with a comprehensive metabolic panel [5].
Medication Disclosures: Inform your doctor about all daily medications, especially aspirin, prescription blood thinners, or over-the-counter NSAIDs like ibuprofen, which can further impact how well your remaining platelets stick together [1].
Maintain Stable Hydration: Ensure you are adequately hydrated before your blood draw, as severe dehydration can falsely concentrate your blood cellular percentages [2].
What Happens During It
The procedure is a routine venipuncture performed by a nurse or trained phlebotomist [5]. An elastic tourniquet is wrapped tightly around your upper arm to fill the targeted vein, the skin is sanitized with an antiseptic alcohol wipe, and a small needle is inserted into the vein [1]. The blood flows into a vacuum collection tube, and the active draw usually concludes in less than 60 seconds [5].
What Happens After It
Immediately following the needle removal, pressure is applied to the puncture site with a sterile gauze pad to promote quick clotting, and an adhesive bandage is applied [5]. Because your platelets may be running low due to your condition, you might need to hold firm pressure on the gauze slightly longer than a standard patient to ensure the bleeding stops completely [4]. Afterward, you are free to immediately leave the clinic, drive home, and continue your day normally [1].
Risks and What to Watch For
A standard CBC draw carries an exceptionally low profile for clinical risk [1]. Potential minor side effects are temporary and include:
Localized bruising, or ecchymosis, or mild soreness around the vein where the needle entered [5].
Brief lightheadedness or a mild vasovagal reaction during or right after the needle stick [2].
Complications to monitor: Because low platelets increase bleeding risks, watch for unexpected pooling of blood under the skin, called a hematoma. Call your provider if you experience rare signs of infection, such as spreading redness, warmth, or swelling at the puncture site [5].
What Results May Mean
While exact reference intervals can vary slightly depending on the specific equipment used by an individual laboratory, a standard normal platelet count ranges from 150,000 to 450,000 platelets per microliter, or mcL, of blood [1].
Normal Range: 150,000 to 450,000 mcL This indicates that your bone marrow is producing an adequate supply of thrombocytes and your spleen is maintaining a healthy storage balance, keeping your baseline clotting defenses stable [2].
Mild to Moderate Thrombocytopenia: 50,000 to 149,000 mcL This is a hallmark signature of cirrhosis and portal hypertension [3]. As my experience reflects, living around 80,000 to 85,000 is highly common. While this range requires careful attention and lifestyle awareness, it generally provides enough density to handle everyday clotting needs without spontaneous bleeding issues [4].
Severe Thrombocytopenia: Below 50,000 mcL This signals a critical reduction in platelet density. At these low thresholds, the trajectory becomes non-linear and high-stakes, as there are simply not enough circulating platelets left to cover the body’s blood vessels safely, drastically increasing the risk of prolonged bleeding from minor cuts or internal strains [4].
Questions to Ask Your Doctor
To help track your personal baseline trends and build your clinical acuity, consider bringing these questions to your next appointment:
What was my exact platelet count on today’s CBC, and how does it compare to my personal baseline over the last year?
Given my current platelet number, are there specific physical restrictions or adjustments I should make to my daily life to avoid injury or bleeding risks?
Does my platelet count indicate that my portal hypertension or spleen size is stable, or is the “jailhouse” trapping more cells than before?
Do I need to take any special precautions or receive a platelet transfusion before undergoing any upcoming dental work or medical procedures?
What specific signs—like certain types of bruising or nosebleeds—should tell me that my platelet levels have dropped into a range that requires immediate care?
Sources
Source 1: Mayo Clinic:Complete Blood Count (CBC) Panel, Platelet References, and Diagnostic Purpose
Source 2: Cleveland Clinic:Understanding Platelets (Thrombocytes), Clotting Function, and Splenic Storage
Source 3: Journal of Hepatology: Consensus Guidelines on the Assessment and Clinical Management of Portal Hypertension and Thrombocytopenia in Liver Cirrhosis
Source 4: The American Journal of Gastroenterology: ACG Clinical Practice Guidance: Managing Clotting Variables, Low Platelets, and Procedural Risks in Advanced Hepatic Diseases
Source 5: National Institutes of Health (NIH) / MedlinePlus: Platelet Count Test Protocols, CBC Reference Ranges, and Low Platelet Evaluations