
Low Sodium Diets
The Moderate vs. Severe Low-Sodium Diet: Navigating the Critical Baseline of Fluid Retention in Cirrhosis
One day your meals are seasoned normally, and you enjoy food without giving the ingredient label a second look. The next, you are handed a strict clinical guideline warning you that a single pinch of salt could trigger an emergency hospital visit for abdominal fluid accumulation.
Dietary modification in advanced liver disease exists on a highly delicate clinical gradient. A moderate sodium restriction (typically capped at 2,000 mg of sodium or 5 grams of table salt per day) is the standard baseline therapy used to minimize systemic fluid accumulation. A severe sodium restriction (dropping below 1,500 mg or 3 grams of salt per day) is a rigid, potentially volatile medical intervention reserved for extreme cases of fluid overload, according to clinical analyses in the MDPI Journal of Clinical Medicine Nutritional Impacts Study. [1, 2]
People frequently look at a low-sodium diet as a simple, risk-free lifestyle choice akin to a standard weight-loss regimen. In reality, shifting from moderate to severe sodium boundaries represents a high-stakes clinical tightrope—one where removing too much salt can trigger a dangerous cascade of muscle wasting, kidney stress, and systemic nutritional failure. [1]
What It Is
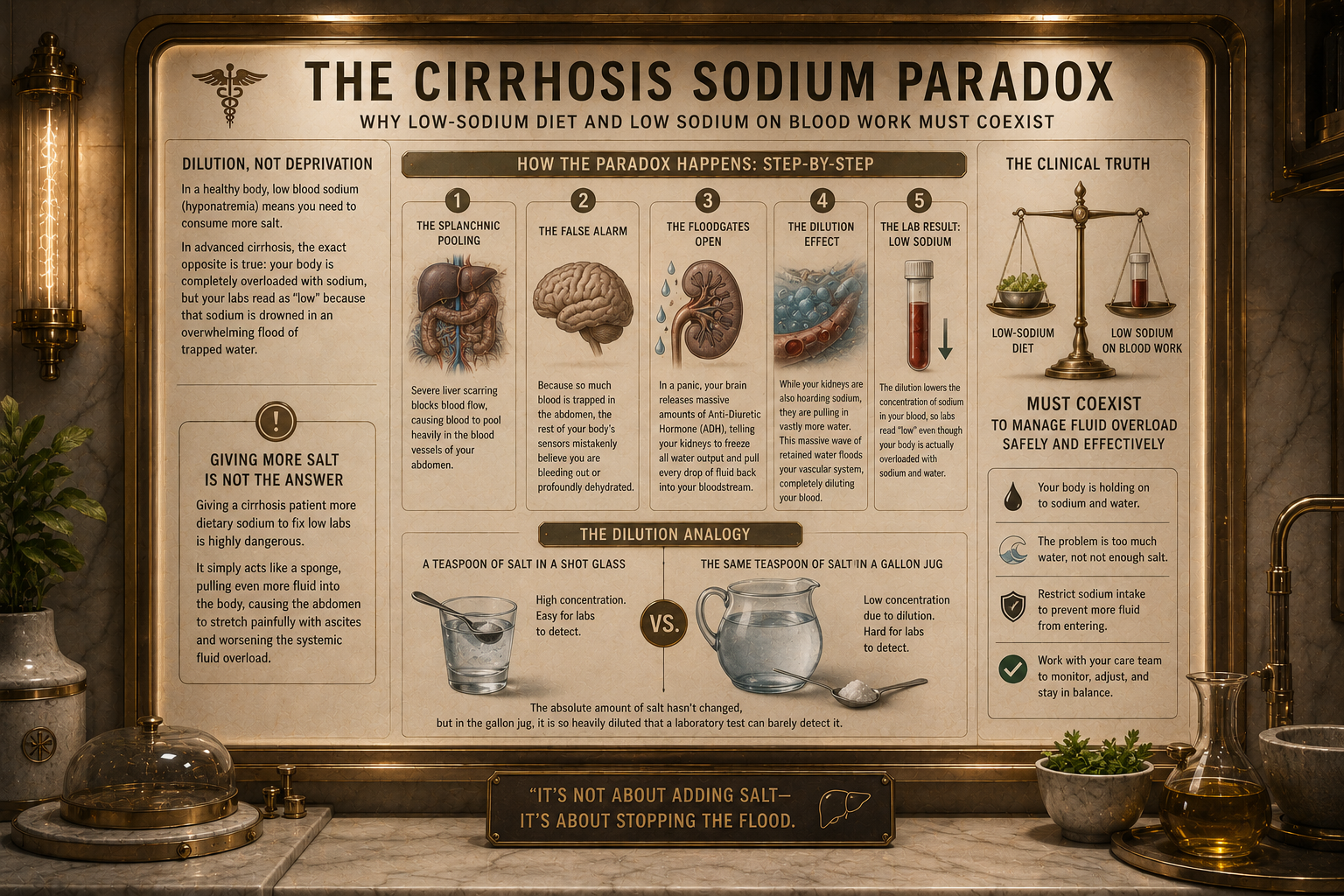
When the liver suffers from advanced cirrhosis, the physical layout of the organ collapses into rigid bands of scar tissue. This structural blockage triggers portal hypertension, forcing blood pressure inside the internal venous highway to skyrocket.
To compensate for this bottleneck, the body releases massive amounts of vasodilators, causing systemic arteries to widen. As detailed in the PubMed Central (PMC) Cirrhosis and Portal Hypertension Framework, the kidneys misinterpret this widened, lower-pressure arterial system as a sign that the body is experiencing massive, life-threatening blood loss. In a desperate bid to save you, the kidneys trigger a profound hormonal panic, aggressively locking onto every molecule of sodium and water they encounter.
To manage this internal fluid flooding, medical teams track sodium intake boundaries across a strict therapeutic spectrum:
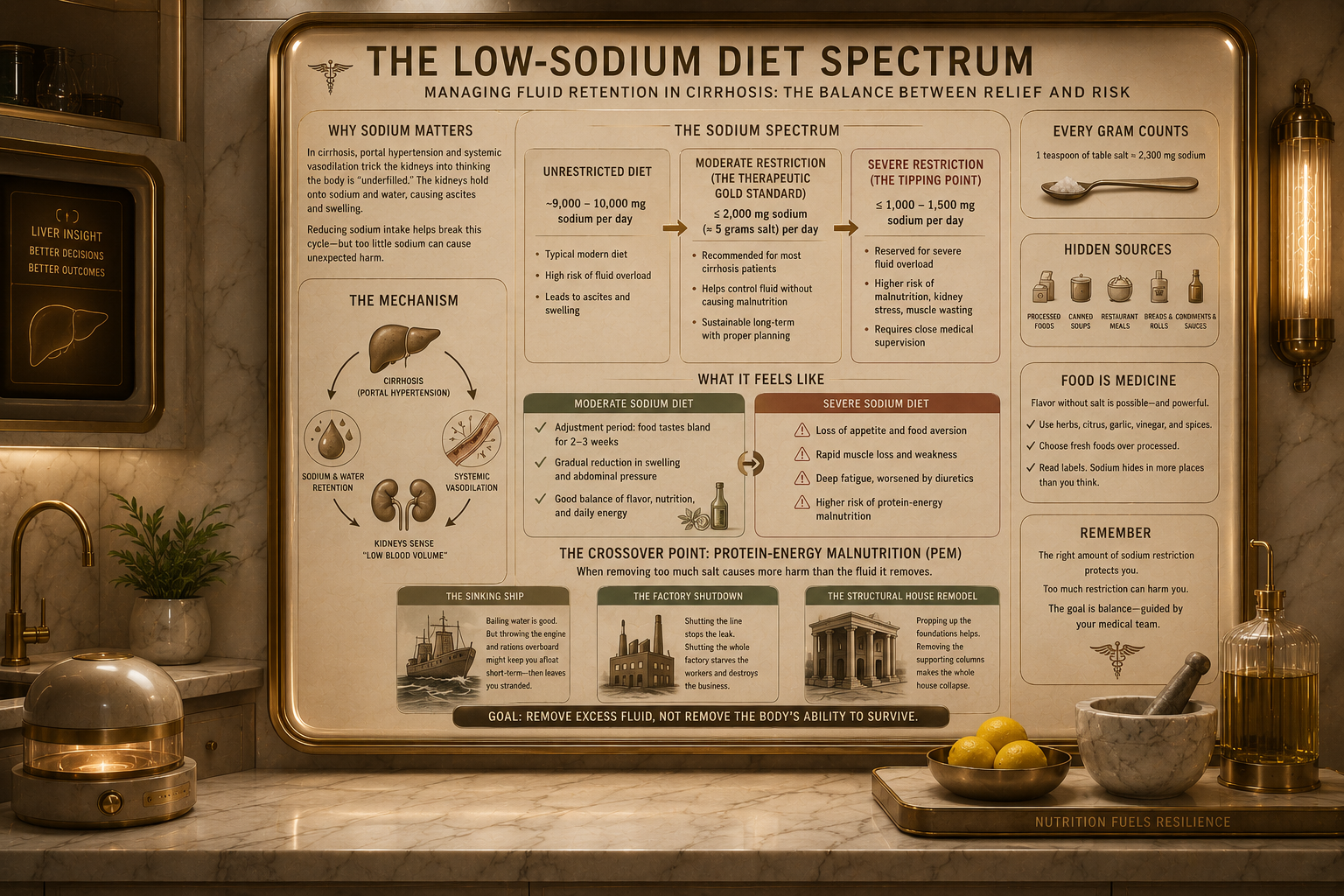
The Unrestricted Baseline: A standard modern diet regularly delivers between 9,000 and 10,000 mg of salt daily, which quickly translates into liters of trapped abdominal fluid (ascites) in a cirrhotic patient.
Moderate Sodium Restriction (The Therapeutic Gold Standard): Guidelines universally recommend capping salt intake at roughly 5 grams per day (equivalent to 2,000 mg of pure sodium). This level is designed to outpace the kidneys' hormonal retention without ruining the flavor of food.
Severe Sodium Restriction (The Tipping Point): Pushing restrictions down into extreme boundaries (less than 1,000 to 1,500 mg of sodium daily) to force rapid fluid drops. While historically common, modern clinical reviews show that this extreme level frequently causes more harm than good. [1, 2, 3]
What It Feels Like
The physical and psychological reality of living on a salt-restricted diet shifts dramatically as the clinical boundaries tighten.
During a Moderate Sodium Diet, you frequently feel:
A profound adjustment period where fresh food tastes entirely bland, flat, or unappealing for the first two to three weeks.
A steady, manageable reduction in the tightness of your skin, accompanied by a noticeable decrease in ankle swelling and abdominal pressure.
A functional balance where, by utilizing natural herbs, citrus, and vinegars, you can still consume enough calories to maintain your baseline physical energy. [1]
When a diet crosses into a Severe Sodium Diet, the daily burden changes completely. Patients experience:
A severe, total loss of appetite (anorexia) driven by profound food aversion and altered taste acuity, making the act of eating feel like a chore.
A frightening, rapid drop in muscle mass and physical strength, particularly in the arms, chest, and shoulders, as the body begins to consume its own muscle for energy.
A deep, constant sense of systemic fatigue and weakness that is exacerbated by the aggressive, overlapping effects of high-dose fluid medications (diuretics). [1, 2, 3]
The Crossover Point: The Shift to Protein-Energy Malnutrition
The transition from a supportive, moderate sodium target to an overly restrictive, severe sodium diet represents a dangerous clinical "crossover point." This is the exact intersection where the mechanical benefit of dropping fluid is entirely wiped out by a catastrophic state known as Protein-Calorie Malnutrition (PCM).
To visualize this crossover point, think of three concrete examples:
The Sinking Ship: In a moderate restriction, you are actively using a bucket to bail water out of a leaking boat—you are controlling the fluid safely. The severe crossover point is like deciding to throw the ship’s heavy backup engine and all food rations overboard just to make the boat lighter. The ship stops sinking for a few hours, but you are now permanently stranded at sea without fuel or nourishment.
The Factory Shutdown: Think of a factory managing a toxic waste spill. A moderate diet is like shutting down the specific assembly line where the leak occurred. The severe crossover point occurs when you panic and cut off the electricity and water to the entire building. The spill stops spreading, but every single worker starves, the machinery rusts, and the entire business permanently goes under.
The Structural House Remodel: Imagine a house with shifting, unstable foundations (the cirrhotic liver). A moderate diet helps prop up the sagging walls. The severe crossover point is equivalent to sandblasting the load-bearing columns of the house to make the rooms look cleaner. The immediate aesthetic improves, but the structural columns become brittle, causing the entire roof to suddenly cave in on itself.
As documented in the PubMed Central (PMC) Liver Cirrhosis Salt Review, crossing this threshold causes a critical clinical shift. Because advanced liver patients require massive amounts of energy to survive, a diet that is too restrictive makes food unpalatable. The patient stops eating, triggers rapid muscle wasting (sarcopenia), and drastically shortens their overall life expectancy. [1]
Things Nobody Explains
1. Severe Salt Restriction Does Not Stop Ascites on Its Own
Many patients assume that if they completely eliminate salt, their abdominal fluid will vanish. This is a false expectation. Clinical data compiled in the PMC Cirrhotic Ascites Trial Review demonstrates that strict sodium restriction alone only successfully eliminates fluid in roughly 10% to 15% of patients. For the vast majority, salt restriction is merely a baseline requirement that must be paired with precise, dual-diuretic therapies to show any true benefit. [1]
2. Cutting Too Much Salt Can Destroy Your Kidneys [1]
When you combine a severe low-sodium diet with powerful fluid pills like furosemide, you can accidentally pull too much fluid out of your blood vessels. The PMC Liver Cirrhosis Salt Review warns that this sudden volume drop starves the kidneys of necessary blood flow, triggering acute kidney injury, dangerous electrolyte imbalances, and a fatal complication called Hepatorenal Syndrome (HRS).
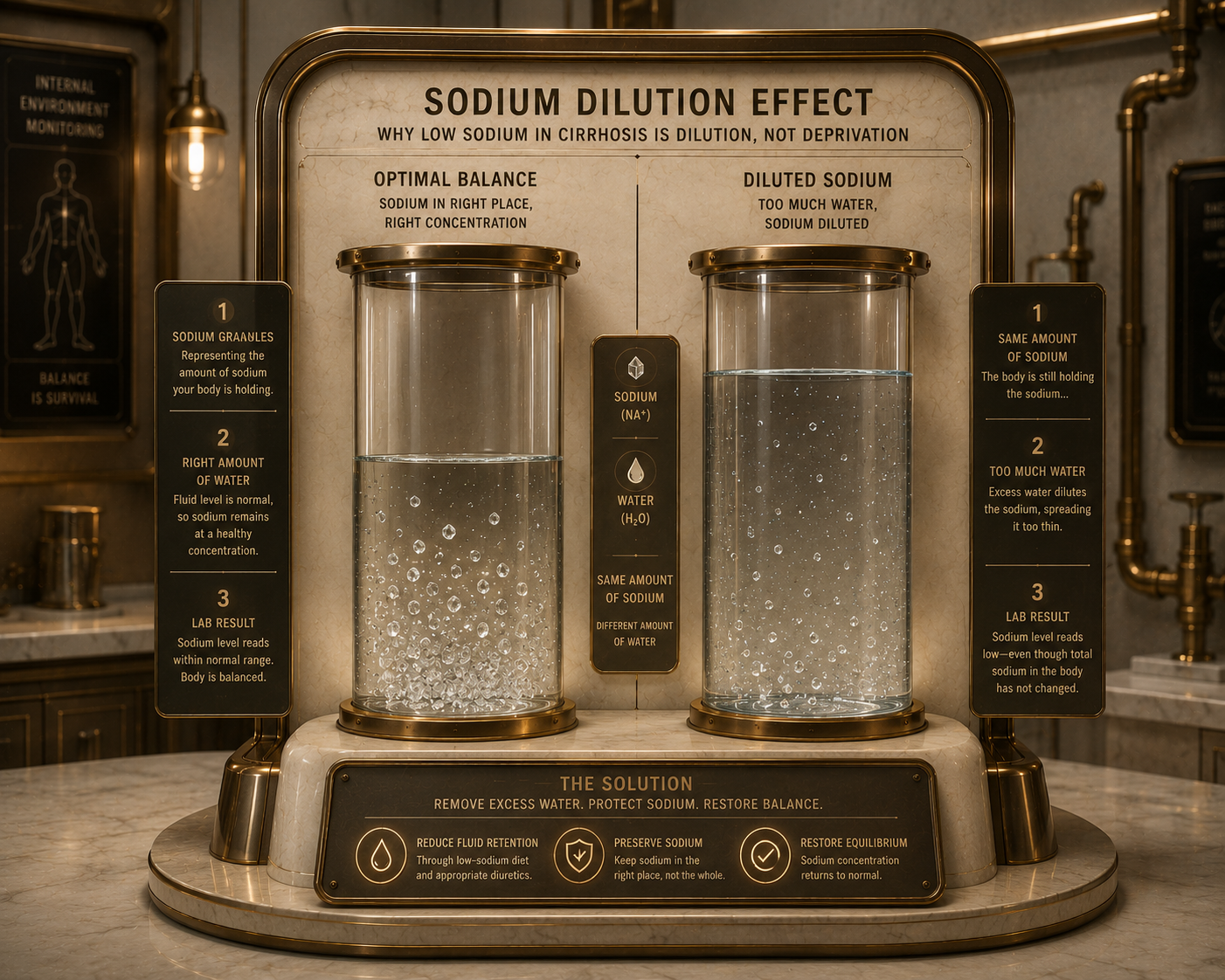
3. It Paradoxically Worsens "Low Sodium" Blood Readings
When advanced liver patients see a low sodium number on their blood work (hyponatremia), their first instinct is to eat more salt, while their second instinct is to cut salt completely. Both are incorrect. As explained in the Journal of Hyponatremia and Malnutrition, low blood sodium in cirrhosis is almost always a dilutionproblem, meaning the body has retained too much water, not too little salt. Restricting salt to severe extremes can stimulate the body to release more antidiuretic hormone, worsening the water retention and dropping blood sodium levels even further. [1]
4. Commercial Salt Substitutes are Hidden Poisons
When transitioning to a low-sodium lifestyle, many patients naturally buy commercial "fake salt" shakers at the grocery store. Nobody explains that these products almost always replace sodium with potassium chloride. In a patient with advanced cirrhosis whose kidneys are already under stress from diuretics, taking in massive, unregulated doses of potassium can cause sudden, fatal cardiac arrhythmias. [1]
What Helps: Clinical Optimization Strategies
The "No-Added-Salt" Protocol: Rather than obsessively weighing milligrams of sodium and causing intense mealtime anxiety, modern hepatology teams recommend focusing on a sustainable "no-added-salt" framework. This means entirely avoiding pre-packaged processed foods, canned goods with added salt, and cured meats, while allowing small, natural amounts of sodium during fresh, home-cooked meal preparation to keep food appetizing.
The Late-Night Supplemental Snack: To counteract the muscle-wasting dangers of a low-sodium diet, guidelines published in the PMC Cirrhosis Nutrition Guide emphasize that patients should consume a dedicated late-night snack rich in Branched-Chain Amino Acids (BCAAs) or high-quality protein. This overnight nutritional bridge stops the body from entering a starvation state during sleep, protecting muscle mass even while sodium is restricted.
Flavor Profiles Without Potassium: To safely restore taste acuity without risking electrolyte shock, clinical dietitians utilize high-acid flavor enhancers. Utilizing fresh lemon zest, lime juice, apple cider vinegars, garlic paste, ginger, and pungent spices allows patients to bypass salt receptors entirely, stimulating salivary flow and preserving appetite safely. [1]
Sources
[1] PubMed Central (PMC):Impacts of salt restriction on nutritional status, sarcopenia, and prognosis in cirrhotic patients with ascites. https://pmc.ncbi.nlm.nih.gov/articles/PMC12261796/
[2] PubMed Central (PMC):Hyponatremia and malnutrition: a comprehensive review. https://pmc.ncbi.nlm.nih.gov/articles/PMC10961272/
[3] PubMed Central (PMC):Dietary salt in liver cirrhosis: With a pinch of salt! https://pmc.ncbi.nlm.nih.gov/articles/PMC10642432/
[4] PubMed Central (PMC):Sodium restriction in patients with cirrhotic ascites: A systematic review. https://pmc.ncbi.nlm.nih.gov/articles/PMC4862086/
[5] PubMed Central (PMC):Hyponatremia in cirrhosis: Pathophysiology and management. https://pmc.ncbi.nlm.nih.gov/articles/PMC4363748/
[6] PubMed Central (PMC):Ascites, Hyponatremia, and Gastroesophageal Variceal Bleeding. https://pmc.ncbi.nlm.nih.gov/articles/PMC9205794/
[7] PubMed Central (PMC):Do Nutritional Interventions Improve the Outcomes of Patients with Cirrhosis? https://pmc.ncbi.nlm.nih.gov/articles/PMC7814292/
Medical Disclaimer & General Guidance
The information provided across these resources is for educational and informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Dietary parameters, fluid adjustments, and electrolyte monitoring in advanced liver disease require individualized oversight by a registered dietitian experienced in hepatology and a certified gastroenterologist. Always seek the direct advice of your physician before changing your daily fluid limits, modifying your salt targets, or introducing any over-the-counter seasoning substitutes.